

Driving with hemianopia, I: Detection performance in a driving simulator
- PMID: 19608541
- PMCID: PMC2783572
- DOI: 10.1167/iovs.09-3799
Driving with hemianopia, I: Detection performance in a driving simulator
Abstract
Purpose: This study was designed to examine the effect of homonymous hemianopia (HH) on detection of pedestrian figures in multiple realistic and hazardous situations within the controlled environment of a driving simulator.
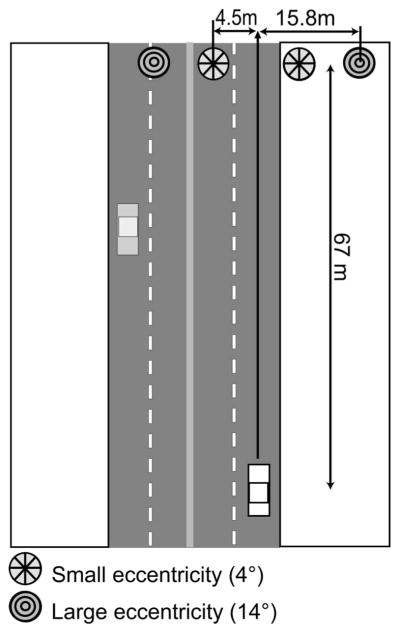
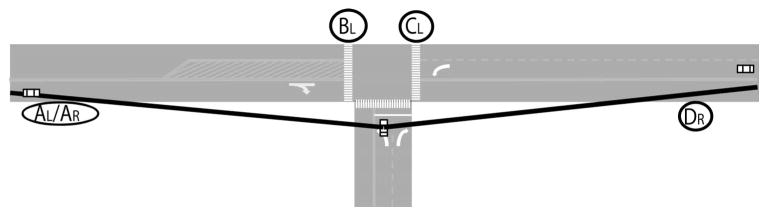
Methods: Twelve people with complete HH and without visual neglect or cognitive decline and 12 matched (age, sex, and years of driving experience) normally sighted (NV) drivers participated. They drove predetermined city and rural highway routes (total, 120 minutes) during which pedestrian figures appeared at random intervals along the roadway (R-Peds; n = 144) and at intersections (I-Peds; n = 10). Detection rates and response times were derived from participant horn presses.
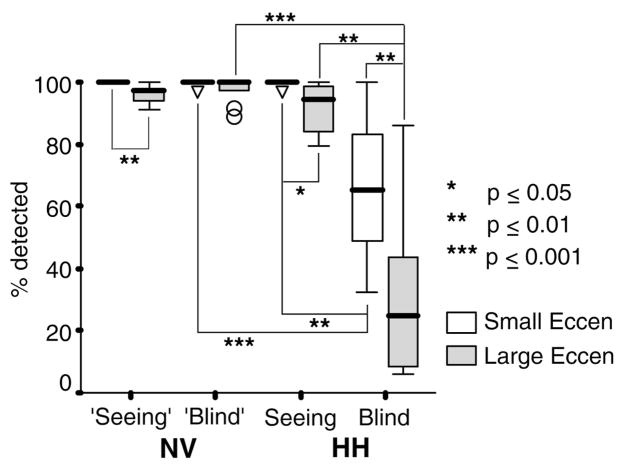
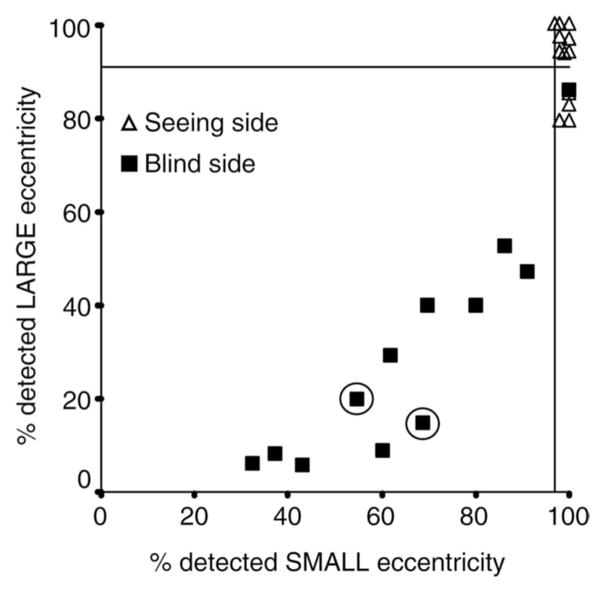
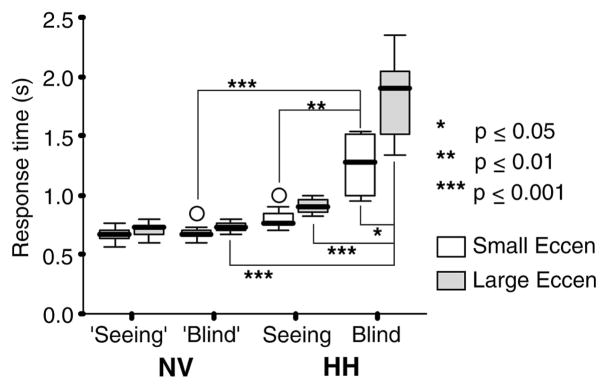
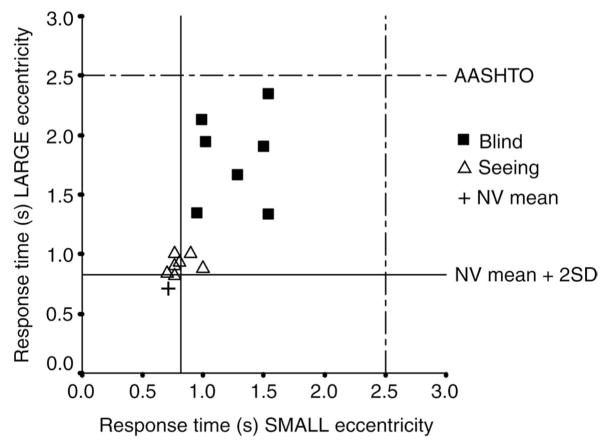
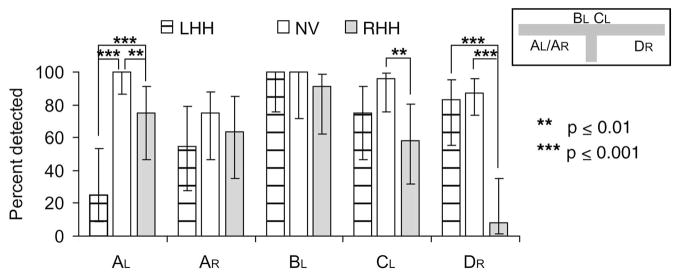
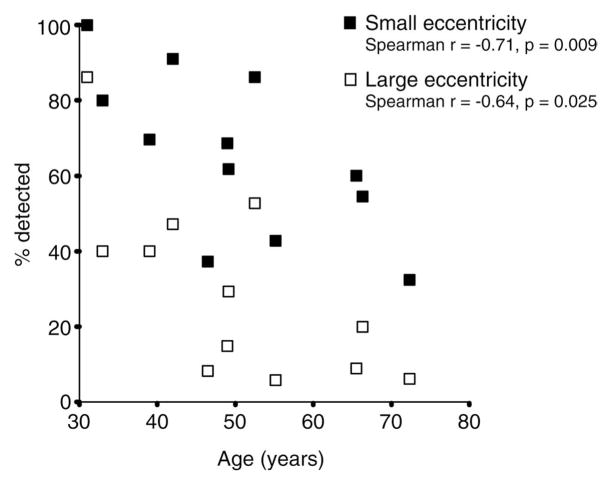
Results: Drivers with HH exhibited significantly (P < 0.001) lower R-Ped detection rates on the blind side than did NV drivers (range, 6%-100%). Detection of I-Peds on the blind side was also poor (8%-55%). Age and blind-side detection rates correlated negatively (Spearman r = -0.71, P = 0.009). Although blind-side response times of drivers with HH were significantly (P < 0.001) longer than those of NV drivers, most were within a commonly used 2.5-second guideline.
Conclusions: Most participants with HH had blind-side detection rates that seem incompatible with safe driving; however, the relationship of our simulator detection performance measures to on-road performance has yet to be established. In determining fitness to drive for people with HH, the results underscore the importance of individualized assessments including evaluations of blind-side hazard detection.
Figures
References
-
- Zhang X, Kedar S, Lynn MJ, Newman NJ, Biousse V. Homonymous hemianopias: clinical-anatomic correlations in 904 cases. Neurology. 2006;66:906–910. - PubMed
-
- Peli E, Peli D. Driving with Confidence: A Practical Guide to Driving with Low Vision. Singapore: World Scientific Publishing; 2002.
-
- Papageorgiou E, Hardiess G, Schaeffel F, et al. Assessment of vision-related quality of life in patients with homonymous visual field defects. Graefes Arch Clin Exp Ophthalmol. 2007;245:1749–1758. - PubMed
-
- de Jong P, Warmink HH. Homonymous hemianopia and driving (letter) Eye. 2003;17:545. - PubMed
-
- Burgess SEP. Homonymous hemianopia and driving: reply. Eye. 2003;17:545–546. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
