

Tragal cartilage in tympanoplasty: anatomic and functional results in 306 cases
- PMID: 19609379
- PMCID: PMC2689610
Tragal cartilage in tympanoplasty: anatomic and functional results in 306 cases
Abstract
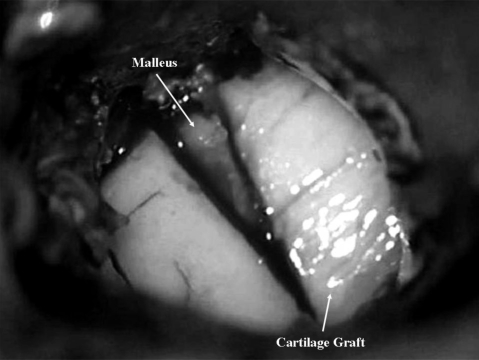
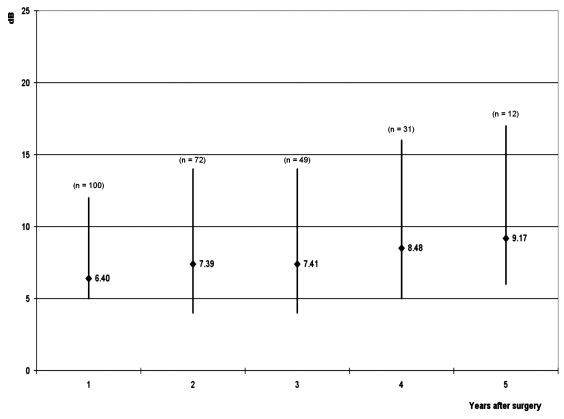
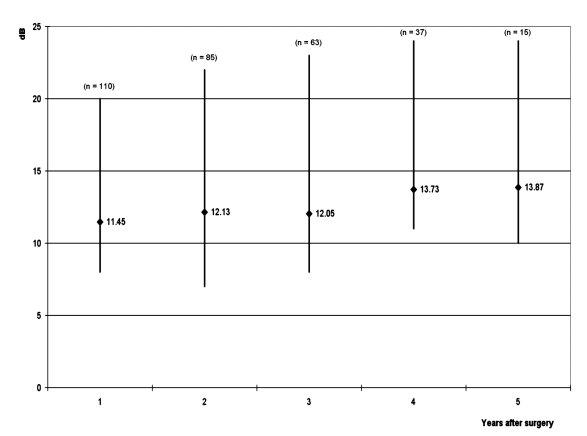
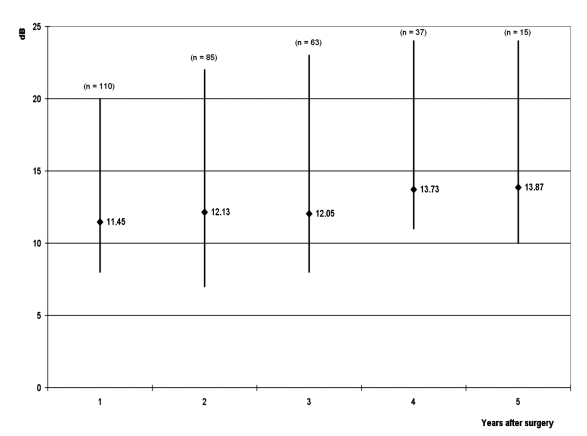
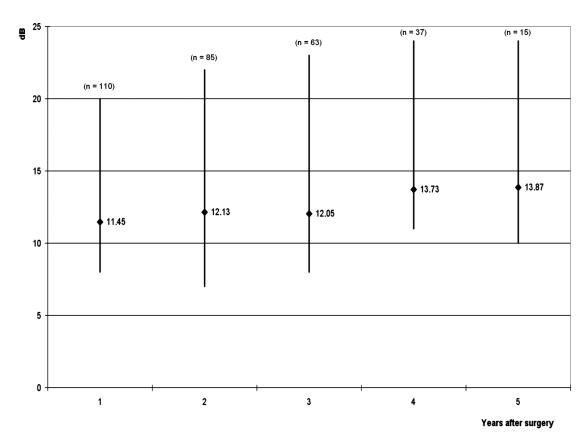
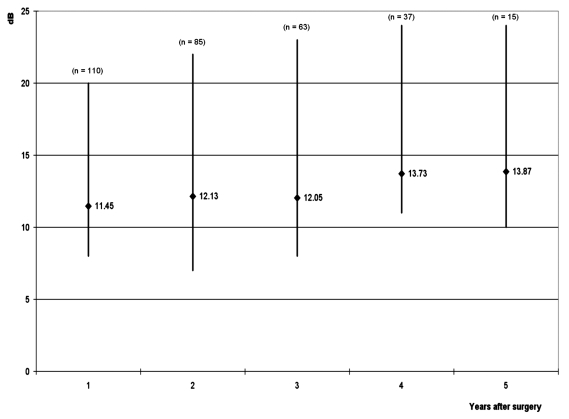
Cartilage is the grafting material of choice in advanced disorders of the middle ear while the indications for its routine use remain controversial due to the possible detrimental effect on post-operative hearing. Aim of the present study was to report personal experience with "tragal cartilage shield" tympanoplasty. The study focused on 306 adult patients (236 primary procedures and 70 revisions from January 2003 to June 2007). Mean post-operative follow-up was 37 months (range 1-66). The following parameters were evaluated: graft take, change between the pre- and post-operative pure-tone average air-bone gap (PTA-ABG), post-operative complications. Graft take was achieved in 304 patients (99.35%) and there were no immediate post-operative complications. The overall average pre-operative pure-tone average air-bone gap was 43.79 +/- 7.07 dB, whereas the post-operative (1 year after surgery) pure-tone average air-bone gap was 10.43 +/- 5.25 dB (p < 0.0001). Statistically significant improvement was observed up to 5 years after surgery. This study reveals that tragal cartilage shield tympanoplasty is a reliable technique, in fact it has a high degree of graft take and hearing results are satisfactory. Furthermore, the cartilage is a satisfactory grafting material because it is easily accessible, easy to adapt, resistant to negative middle ear pressures, stable, elastic, well tolerated by the middle ear, resistant to resorption. Therefore, we also recommend its use in less severe middle ear disorders, in which the functional outcome is more essential.
La cartilagine rappresenta l’innesto di scelta nelle patologie complicate dell’orecchio medio, mentre le indicazioni per un suo utilizzo di routine rimangono ancora controverse a causa dei presunti effetti negativi sui risultati uditivi. In questo studio riferiamo la nostra esperienza nella timpanoplastica con cartilagine del trago modellata a scudo (Cartilage Shield). Viene riportata la nostra esperienza su 306 pazienti (236 procedure primarie e 70 revisioni, da gennaio 2003 a giugno 2007). Il follow-up post-operatorio medio è stato di 37 mesi (range, 1-66 mesi). Abbiamo valutato i seguenti parametri: attecchimento dell’innesto, modifiche del gap medio via aerea-via ossea prima e dopo l’intervento, complicanze postoperatorie. L’attecchimento dell’innesto è stato ottenuto in 304 pazienti (99,35%) e non si sono registrate complicanze postoperatorie immediate. Il gap medio complessivo via aerea-via ossea prima e ad un anno dopo l’intervento è stato rispettivamente di 43,79 ± 7,07 dB e di 10,43 ± 5,25 dB (p < 0,0001). Miglioramenti significativi sono stati osservati fino a 5 anni dopo l’intervento. Questo studio dimostra che la tecnica della timpanoplastica con cartilagine del trago modellata a scudo è affidabile sia per l’alto tasso di attecchimento dell’innesto sia per i soddisfacenti risultati uditivi. Inoltre la cartilagine si è rivelata un adeguato materiale di innesto perché è facilmente accessibile, adatta al modellamento, resistente alle pressioni negative dell’orecchio medio, stabile, elastica, ben tollerata, resistente al riassorbimento. Per tutti questi motivi raccomandiamo l’utilizzo della cartilagine anche nelle patologie meno severe dell’orecchio medio, laddove l’aspettativa di un buon risultato funzionale è maggiore.
Keywords: Chronic otitis; Middle ear; Shield; Tragal cartilage; Tympanoplasty.
Figures
References
-
- Zoellner F. The principles of plastic surgery of the sound-conducting apparatus. J Laryngol Otol 1955;69:567-9. - PubMed
-
- Wullstein HL. Functional operations in the middle ear with split-thickness skin graft. Arch Otorhinolaryngol 1952;161:422-35.
-
- Heermann H. Tympanic membrane plastic with temporal fascia. Hals Nas Ohren 1960;9:136-9.
-
- Shea JJ. Vein graft closure of eardrum perforations. J Laryngol Otol 1960;74:358-62. - PubMed
-
- Preobrazhenski TB, Rugov AA. The employment of preserved dura mater graft in tympanoplasty. Vestn Otorinolaringol 1965;5:38-42. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous