

Antiphospholipid antibodies induce a pro-inflammatory response in first trimester trophoblast via the TLR4/MyD88 pathway
- PMID: 19614626
- PMCID: PMC2772057
- DOI: 10.1111/j.1600-0897.2009.00717.x
Antiphospholipid antibodies induce a pro-inflammatory response in first trimester trophoblast via the TLR4/MyD88 pathway
Abstract
Problem: Women with antiphospholipid antibodies (aPL) are at risk for recurrent miscarriage, pre-eclampsia, and pre-term labor. aPL target the placenta directly by binding to beta(2)-glycoprotein I (beta(2)GPI) expressed on the surface of trophoblast cells. The objective of this study was to determine the effects of aPL on trophoblast function and the mechanisms involved.
Method of study: First trimester trophoblast cells were treated with anti-beta(2)GPI monoclonal antibodies and patient-derived aPL, after which cell survival and function was evaluated.
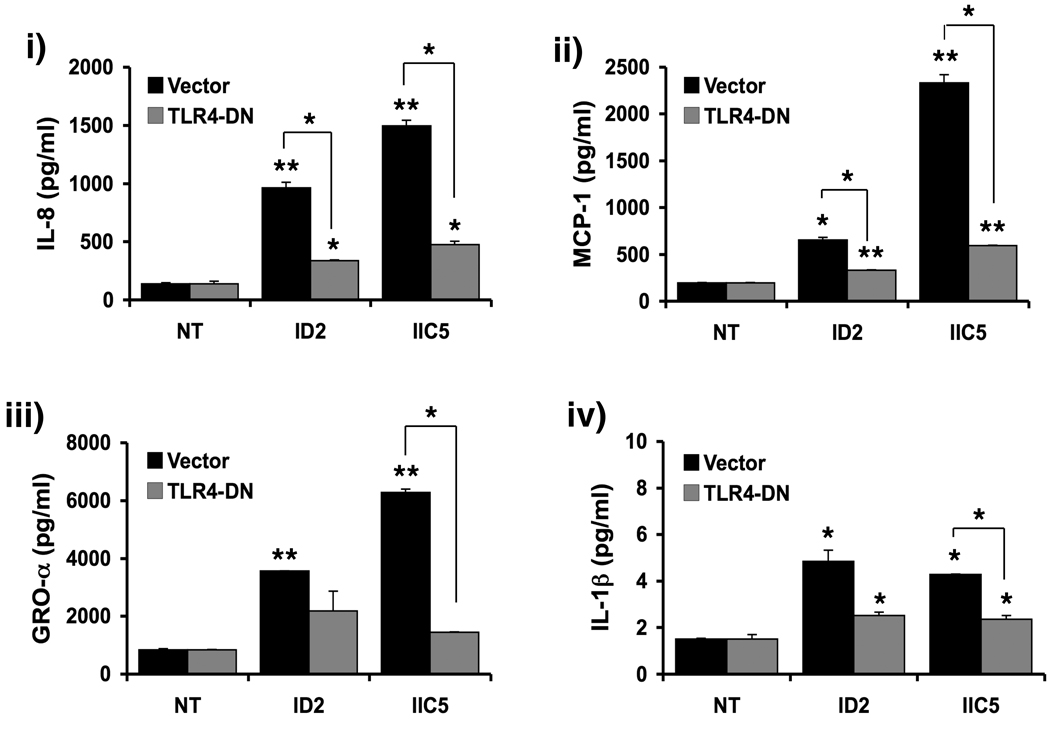
Results: We report that anti-beta(2)GPI antibodies trigger an inflammatory response in trophoblast, characterized by increased secretion of interleukin (IL)-8, MCP-1, GRO-alpha, and IL-1beta, and that this occurs in a TLR-4/MyD88-dependent manner. At high concentrations, these antibodies also induce caspase-mediated cell death. This was attenuated upon disabling of the MyD88 pathway, suggesting that anti-beta(2)GPI-induced inflammatory mediators compromise trophoblast survival by acting in an autocrine/paracrine manner. Enhanced IL-8, GRO-alpha, and IL-1beta secretion also occurred when trophoblast cells were incubated with antibodies from patients with antiphospholipid syndrome. Heparin, which acts as a pro-survival factor in human trophoblast, attenuated the anti-beta(2)GPI antibody-mediated cell death, and also the pro-inflammatory response, but only at high concentrations.
Conclusion: These findings demonstrate that aPL triggers a placental inflammatory response via the TLR-4/MyD88 pathway, which in turn compromises trophoblast survival. Thus, the TLR-4/MyD88 pathway may provide a new therapeutic target to improve pregnancy outcome in antiphospholipid syndrome patients.
Figures







References
-
- D'Cruz DP, Khamashta MA, Hughes GR. Systemic lupus erythematosus. Lancet. 2007;369:587–596. - PubMed
-
- Valesini G, Alessandri C. New facet of antiphospholipid antibodies. Ann N Y Acad Sci. 2005;1051:487–497. - PubMed
-
- Rai RS, Regan L, Clifford K, Pickering W, Dave M, Mackie I, McNally T, Cohen H. Antiphospholipid antibodies and beta 2-glycoprotein-I in 500 women with recurrent miscarriage: results of a comprehensive screening approach. Hum Reprod. 1995;10:2001–2005. - PubMed
-
- Regan L, Rai R. Epidemiology and the medical causes of miscarriage. Baillieres Best Pract Res Clin Obstet Gynaecol. 2000;14:839–854. - PubMed
-
- Cervera R, Piette JC, Font J, Khamashta MA, Shoenfeld Y, Camps MT, Jacobsen S, Lakos G, Tincani A, Kontopoulou-Griva I, Galeazzi M, Meroni PL, Derksen RH, de Groot PG, Gromnica-Ihle E, Baleva M, Mosca M, Bombardieri S, Houssiau F, Gris JC, Quere I, Hachulla E, Vasconcelos C, Roch B, Fernandez-Nebro A, Boffa MC, Hughes GR, Ingelmo M. Antiphospholipid syndrome: clinical and immunologic manifestations and patterns of disease expression in a cohort of 1,000 patients. Arthritis Rheum. 2002;46:1019–1027. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
