

Utility of lead aVR for identifying the culprit lesion in acute myocardial infarction
- PMID: 19614632
- PMCID: PMC6932033
- DOI: 10.1111/j.1542-474X.2009.00300.x
Utility of lead aVR for identifying the culprit lesion in acute myocardial infarction
Abstract
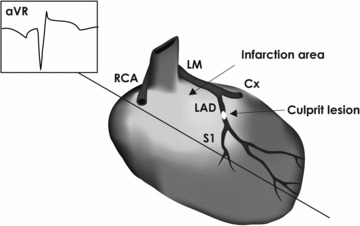
Background: Lead aVR is a neglected, however, potentially useful tool in electrocardiography. Our aim was to evaluate its value in clinical practice, by reviewing existing literature regarding its utility for identifying the culprit lesion in acute myocardial infarction (AMI).
Methods: Based on a systematic search strategy, 16 studies were assessed with the intent to pool data; diagnostic test rates were calculated as key results.
Results: Five studies investigated if ST-segment elevation (STE) in aVR is valuable for the diagnosis of left main stem stenosis (LMS) in non-ST-segment AMI (NSTEMI). The studies were too heterogeneous to pool, but the individual studies all showed that STE in aVR has a high negative predictive value (NPV) for LMS. Six studies evaluated if STE in aVR is valuable for distinguishing proximal from distal lesions in the left anterior descending artery (LAD) in anterior ST-segment elevation AMI (STEMI). Pooled data showed a sensitivity of 47%, a specificity of 96%, a positive predicative value (PPV) of 91% and a NPV of 69%. Five studies examined if ST-segment depression (STD) in lead aVR is valuable for discerning lesions in the circumflex artery from those in the right coronary artery in inferior STEMI. Pooled data showed a sensitivity of 37%, a specificity of 86%, a PPV of 42%, and an NPV of 83%.
Conclusion: The absence of aVR STE appears to exclude LMS as the underlying cause in NSTEMI; in the context of anterior STEMI, its presence indicates a culprit lesion in the proximal segment of LAD.
Figures

Similar articles
-
The Value of Lead aVR ST Segment Changes in Localizing Culprit Lesion in Acute Inferior Myocardial Infarction and Its Prognostic Impact.Ann Noninvasive Electrocardiol. 2016 Jul;21(4):389-96. doi: 10.1111/anec.12324. Epub 2015 Nov 2. Ann Noninvasive Electrocardiol. 2016. PMID: 26523845 Free PMC article.
-
Improved detection of acute myocardial infarction in patients with chest pain and significant left main stem coronary stenosis.QJM. 2012 Feb;105(2):127-35. doi: 10.1093/qjmed/hcr134. Epub 2011 Sep 3. QJM. 2012. PMID: 21890878
-
Acute anterior wall myocardial infarction entailing ST-segment elevation in lead V3R, V1 or aVR: electrocardiographic and angiographic correlations.J Electrocardiol. 2008 Jul-Aug;41(4):329-34. doi: 10.1016/j.jelectrocard.2007.12.004. Epub 2008 Mar 19. J Electrocardiol. 2008. PMID: 18353349
-
Identifying the culprit artery via 12-lead electrocardiogram in inferior wall ST-segment elevation myocardial infarction: A meta-analysis.Ann Noninvasive Electrocardiol. 2023 Jan;28(1):e13016. doi: 10.1111/anec.13016. Epub 2022 Nov 1. Ann Noninvasive Electrocardiol. 2023. PMID: 36317727 Free PMC article. Review.
-
Prognostic implications of ST-segment elevation in lead aVR in patients with acute coronary syndrome: A meta-analysis.Ann Noninvasive Electrocardiol. 2021 Jan;26(1):e12811. doi: 10.1111/anec.12811. Epub 2020 Oct 15. Ann Noninvasive Electrocardiol. 2021. PMID: 33058358 Free PMC article.
Cited by
-
ST Segment Elevation in aVR: Clinical Significance in Acute Coronary Syndrome.Clin Med Insights Case Rep. 2013 Mar 21;6:41-5. doi: 10.4137/CCRep.S11261. Print 2013. Clin Med Insights Case Rep. 2013. PMID: 23589701 Free PMC article.
-
The Value of Lead aVR ST Segment Changes in Localizing Culprit Lesion in Acute Inferior Myocardial Infarction and Its Prognostic Impact.Ann Noninvasive Electrocardiol. 2016 Jul;21(4):389-96. doi: 10.1111/anec.12324. Epub 2015 Nov 2. Ann Noninvasive Electrocardiol. 2016. PMID: 26523845 Free PMC article.
-
Combining electrocardiographic criteria for predicting acute total left main coronary artery occlusion.Front Cardiovasc Med. 2022 Aug 11;9:936687. doi: 10.3389/fcvm.2022.936687. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36035902 Free PMC article.
-
Left main coronary artery disease: A review of the spectrum of noninvasive diagnostic modalities.J Nucl Cardiol. 2016 Dec;23(6):1411-1429. doi: 10.1007/s12350-015-0152-1. Epub 2015 Oct 20. J Nucl Cardiol. 2016. PMID: 26487011 Review.
-
Acute myocardial infarction due to left main coronary artery disease in men and women: does ST-segment elevation matter?Arch Med Sci. 2015 Dec 10;11(6):1197-204. doi: 10.5114/aoms.2015.56345. Epub 2015 Dec 11. Arch Med Sci. 2015. PMID: 26788080 Free PMC article.
References
-
- Myers GB, Klein HA, Hiratzka T. Correlation of electrocardiographic and pathologic findings in posterolateral infarction. Am Heart J 1949;38:837–862. - PubMed
-
- Goldberger E. A simple, indifferent, electrocardiographic electrode of zero potential and a technique of obtaining augmented, unipolar, extremity leads. Am Heart J 1942;23:483–493.
-
- Pahlm US, Pahlm O, Wagner GS. The standard 11‐lead ECG. Neglect of lead aVR in the classical limb lead display. J Electrocardiol 1996;29(Suppl):270–274. - PubMed
-
- Gorgels AP, Engelen DJ, Wellens HJ. Lead aVR, a mostly ignored but very valuable lead in clinical electrocardiography. J Am Coll Cardiol 2001;38:1355–1356. - PubMed
-
- Staggs SE, Glancy DL. Clinical uses of electrocardiographic lead aVR. J La State Med Soc 2005;157:308–317. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
