

Design of a complex virtual reality simulation to train finger motion for persons with hemiparesis: a proof of concept study
- PMID: 19615045
- PMCID: PMC2729310
- DOI: 10.1186/1743-0003-6-28
Design of a complex virtual reality simulation to train finger motion for persons with hemiparesis: a proof of concept study
Abstract
Background: Current neuroscience has identified rehabilitation approaches with the potential to stimulate adaptive changes in the brains of persons with hemiparesis. These approaches include, intensive task-oriented training, bimanual activities and balancing proximal and distal upper extremity interventions to reduce competition between these segments for neural territory.
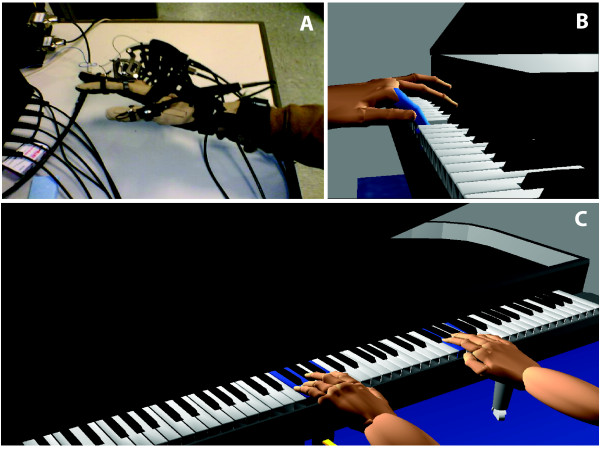
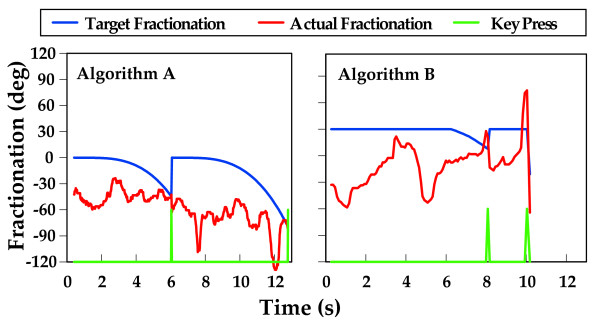
Methods: This paper describes the design and feasibility testing of a robotic/virtual environment system designed to train the hand and arm of persons with hemiparesis. The system employs a simulated piano that presents visual, auditory and tactile feedback comparable to an actual piano. Arm tracking allows patients to train both the arm and hand as a coordinated unit, emphasizing the integration of both transport and manipulation phases. The piano trainer includes songs and scales that can be performed with one or both hands. Adaptable haptic assistance is available for more involved subjects. An algorithm adjusts task difficulty in proportion to subject performance. A proof of concept study was performed on four subjects with upper extremity hemiparesis secondary to chronic stroke to establish: a) the safety and feasibility of this system and b) the concurrent validity of robotically measured kinematic and performance measures to behavioral measures of upper extremity function.
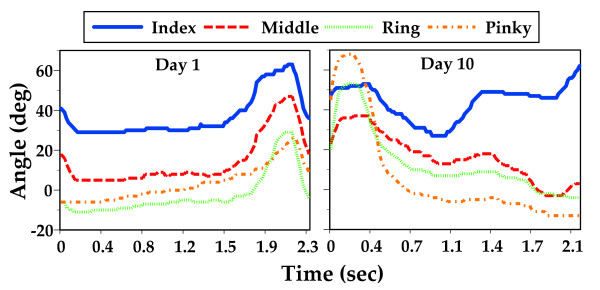
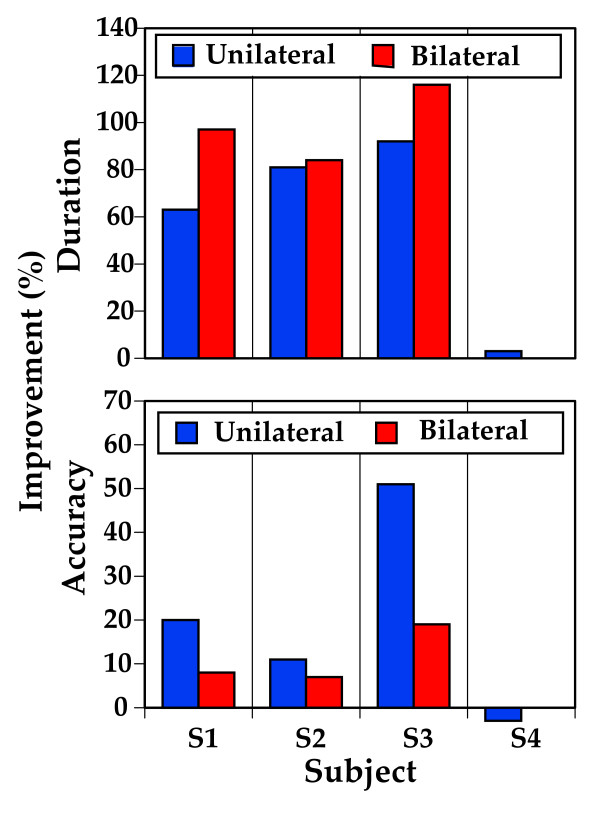
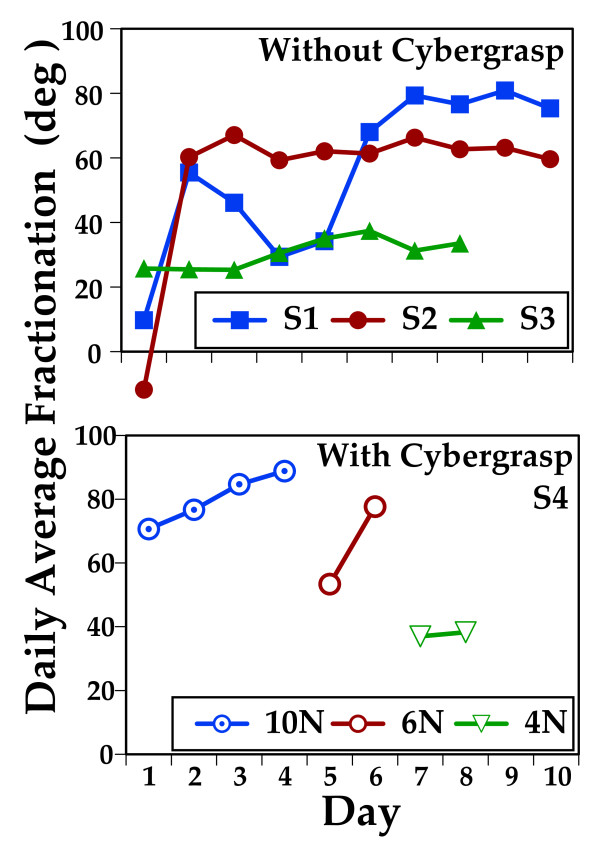
Results: None of the subjects experienced adverse events or responses during or after training. As a group, the subjects improved in both performance time and key press accuracy. Three of the four subjects demonstrated improvements in fractionation, the ability to move each finger individually. Two subjects improved their aggregate time on the Jebsen Test of Hand Function and three of the four subjects improved in Wolf Motor Function Test aggregate time.
Conclusion: The system designed in this paper has proven to be safe and feasible for the training of hand function for persons with hemiparesis. It features a flexible design that allows for the use and further study of adjustments in point of view, bilateral and unimanual treatment modes, adaptive training algorithms and haptically rendered collisions in the context of rehabilitation of the hemiparetic hand.
Figures
References
-
- American Heart Association
-
- Gowland C, deBruin H, Basmajian JV, Plews N, Burcea I. Agonist and antagonist activity during voluntary upper-limb movement in patients with stroke. Phys Ther. 1992;72:624–633. - PubMed
-
- Mahncke HW, Bronstone A, Merzenich MM. Brain plasticity and functional losses in the aged: scientific bases for a novel intervention. Prog Brain Res. 2006;157:81–109. - PubMed
-
- Schneider S, Schonle PW, Altenmuller E, Munte TF. Using musical instruments to improve motor skill recovery following a stroke. J Neurol. 2007;254:1339–1346. - PubMed
-
- Huang H, Chen Y, Xu W, Sundaram H, Olson L, Ingalls T, Rikakis T, He J. Novel design of interactive multimodal biofeedback system for neurorehabilitation. Conf Proc IEEE Eng Med Biol Soc. 2006;1:4925–4928. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
