

Chest tomosynthesis: technical principles and clinical update
- PMID: 19616909
- PMCID: PMC3693857
- DOI: 10.1016/j.ejrad.2009.05.054
Chest tomosynthesis: technical principles and clinical update
Abstract
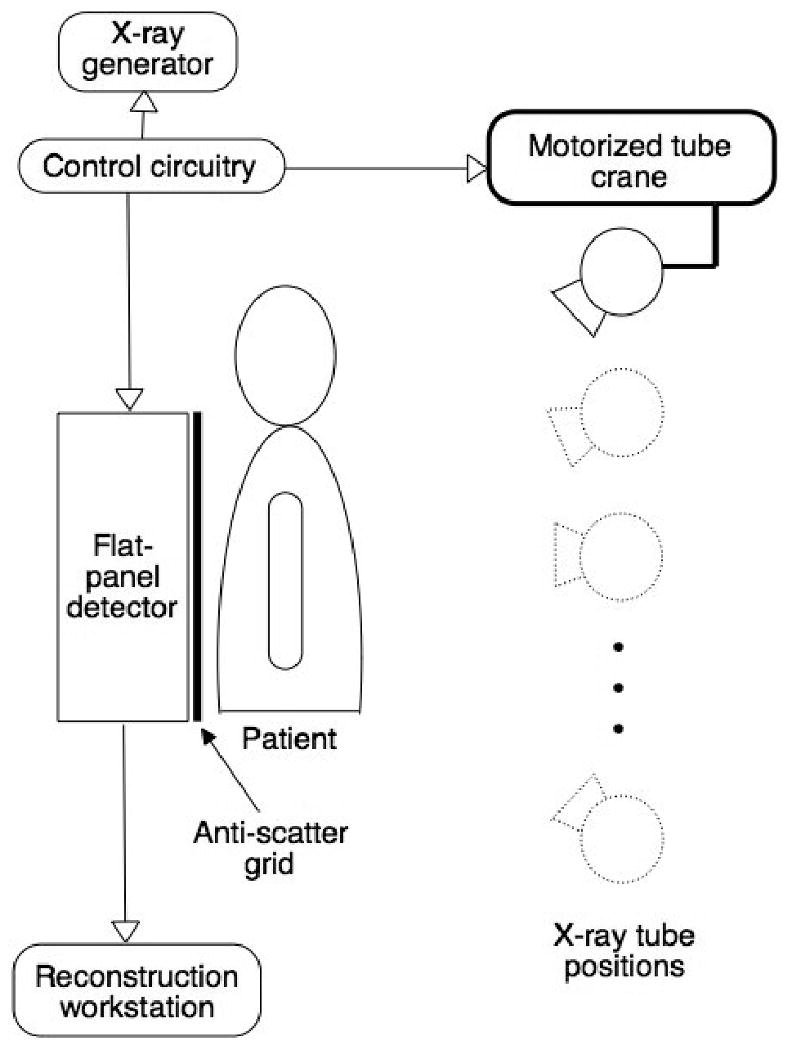
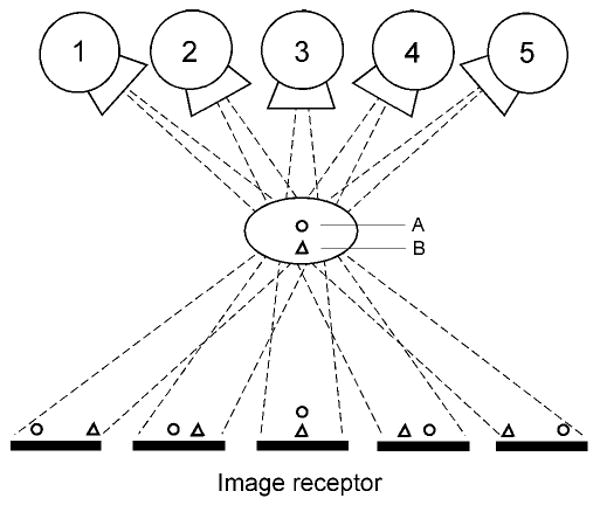
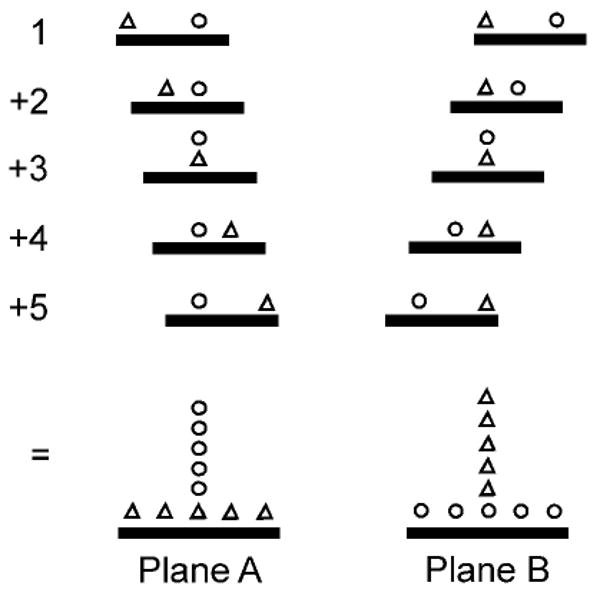
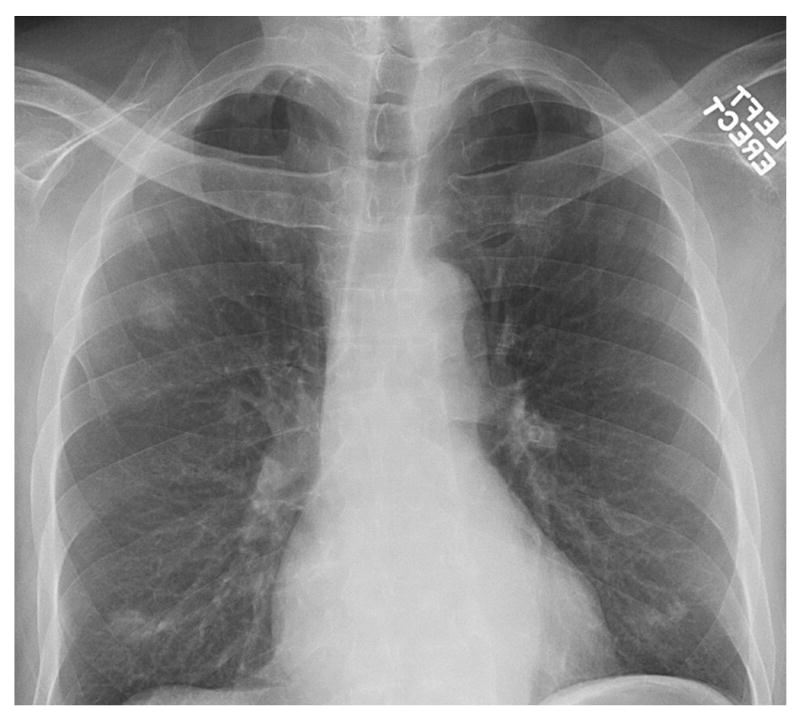
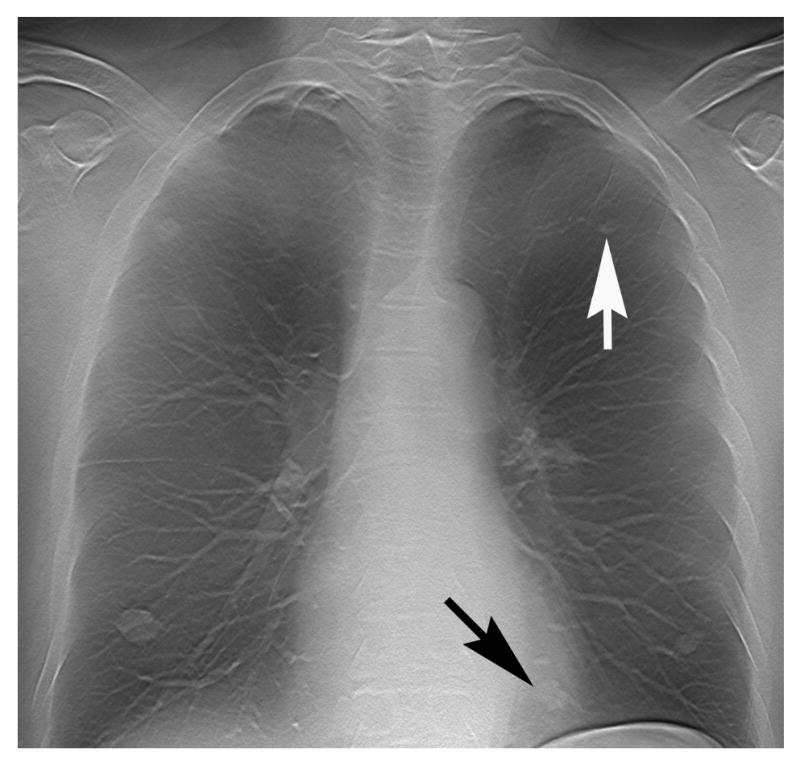
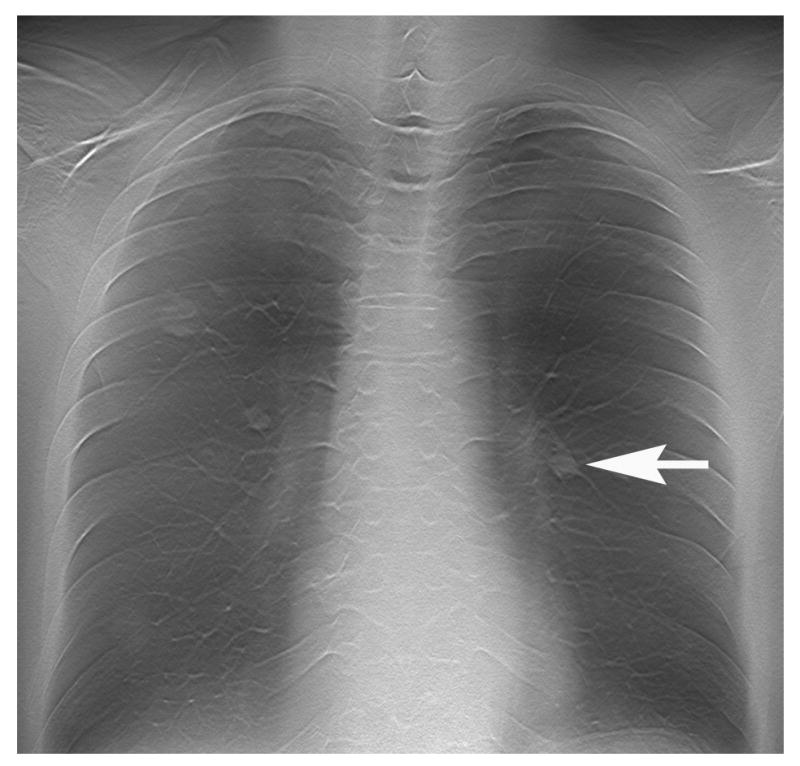
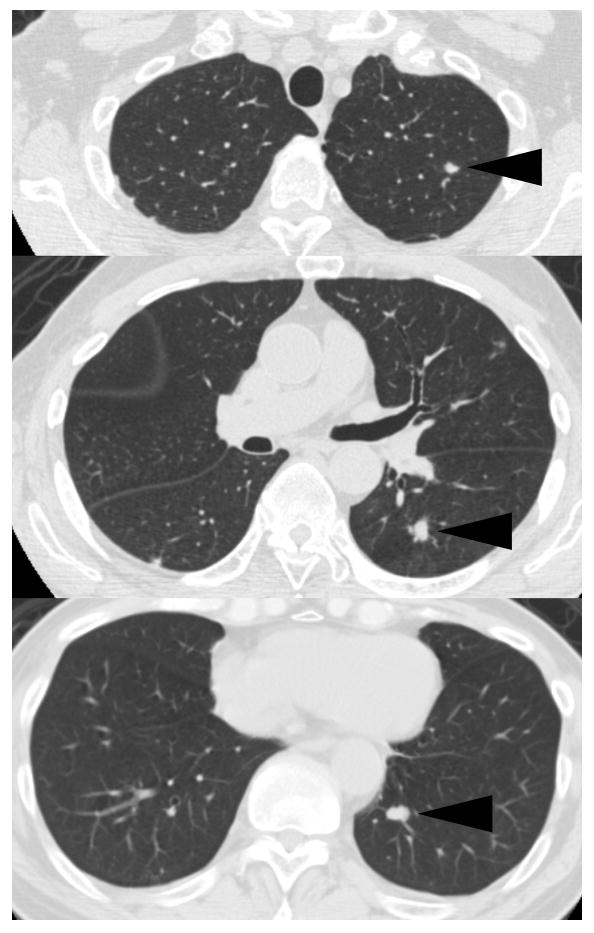
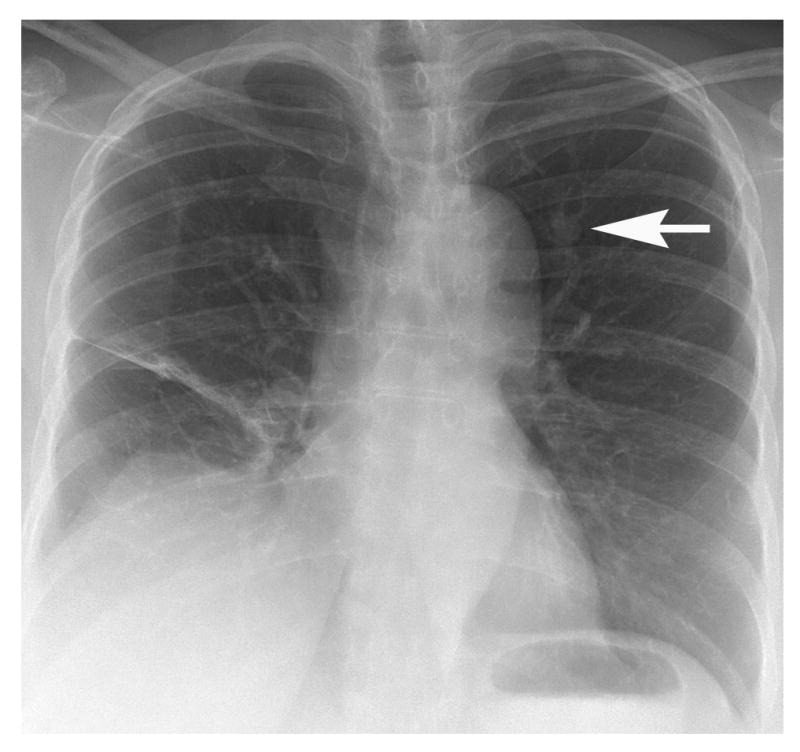
Digital tomosynthesis is a radiographic technique that can produce an arbitrary number of section images of a patient from a single pass of the X-ray tube. It utilizes a conventional X-ray tube, a flat-panel detector, a computer-controlled tube mover, and special reconstruction algorithms to produce section images. While it does not have the depth resolution of computed tomography (CT), tomosynthesis provides some of the tomographic benefits of CT but at lower cost and radiation dose than CT. Compared to conventional chest radiography, chest tomosynthesis results in improved visibility of normal structures such as vessels, airway and spine. By reducing visual clutter from overlying normal anatomy, it also enhances detection of small lung nodules. This review article outlines the components of a tomosynthesis system, discusses results regarding improved lung nodule detection from the recent literature, and presents examples of nodule detection from a clinical trial in human subjects. Possible implementation strategies for use in clinical chest imaging are discussed.
Figures
Similar articles
-
Digital tomosynthesis of the chest.J Thorac Imaging. 2008 May;23(2):86-92. doi: 10.1097/RTI.0b013e318173e162. J Thorac Imaging. 2008. PMID: 18520565 Review.
-
Digital x-ray tomosynthesis: current state of the art and clinical potential.Phys Med Biol. 2003 Oct 7;48(19):R65-106. doi: 10.1088/0031-9155/48/19/r01. Phys Med Biol. 2003. PMID: 14579853 Review.
-
Chest tomosynthesis: technical and clinical perspectives.Semin Respir Crit Care Med. 2014 Feb;35(1):17-26. doi: 10.1055/s-0033-1363448. Epub 2014 Jan 30. Semin Respir Crit Care Med. 2014. PMID: 24481756
-
X-ray tomosynthesis: a review of its use for breast and chest imaging.Radiat Prot Dosimetry. 2010 Apr-May;139(1-3):100-7. doi: 10.1093/rpd/ncq099. Epub 2010 Mar 16. Radiat Prot Dosimetry. 2010. PMID: 20233756 Review.
-
Digital tomosynthesis of the chest for lung nodule detection: interim sensitivity results from an ongoing NIH-sponsored trial.Med Phys. 2008 Jun;35(6):2554-7. doi: 10.1118/1.2937277. Med Phys. 2008. PMID: 18649488 Free PMC article. Clinical Trial.
Cited by
-
Stationary intraoral digital tomosynthesis using a carbon nanotube X-ray source array.Dentomaxillofac Radiol. 2015;44(9):20150098. doi: 10.1259/dmfr.20150098. Epub 2015 Jun 19. Dentomaxillofac Radiol. 2015. PMID: 26090933 Free PMC article.
-
Multi-Institutional Evaluation of Digital Tomosynthesis, Dual-Energy Radiography, and Conventional Chest Radiography for the Detection and Management of Pulmonary Nodules.Radiology. 2017 Jan;282(1):236-250. doi: 10.1148/radiol.2016150497. Epub 2016 Jul 19. Radiology. 2017. PMID: 27439324 Free PMC article. Clinical Trial.
-
Model evaluation of rapid 4-dimensional lung tomosynthesis.Adv Radiat Oncol. 2018 Mar 8;3(3):431-438. doi: 10.1016/j.adro.2018.03.001. eCollection 2018 Jul-Sep. Adv Radiat Oncol. 2018. PMID: 30202810 Free PMC article.
-
Digital Tomosynthesis Applications in Pediatric Orthopedic Imaging: A Case Series.Mo Med. 2018 Jul-Aug;115(4):344-348. Mo Med. 2018. PMID: 30228765 Free PMC article.
-
EFFECT OF RADIATION DOSE LEVEL ON ACCURACY AND PRECISION OF MANUAL SIZE MEASUREMENTS IN CHEST TOMOSYNTHESIS EVALUATED USING SIMULATED PULMONARY NODULES.Radiat Prot Dosimetry. 2016 Jun;169(1-4):188-98. doi: 10.1093/rpd/ncw041. Epub 2016 Mar 17. Radiat Prot Dosimetry. 2016. PMID: 26994093 Free PMC article.
References
-
- McAdams HP, Samei E, Dobbins J, 3rd, Tourassi GD, Ravin CE. Recent advances in chest radiography. Radiology. 2006;241:663–683. - PubMed
-
- Pascoal A, Lawinski CP, Mackenzie A, Tabakov S, Lewis CA. Chest radiography: a comparison of image quality and effective dose using four digital systems. Radiat Prot Dosimetry. 2005;114:273–277. - PubMed
-
- Ricke J, Fischbach F, Freund T, et al. Clinical results of CsI-detector-based dual-exposure dual energy in chest radiography. European Radiology. 2003;13:2577–2582. - PubMed
-
- MacMahon H, Li F, Engelmann R, Roberts R, Armato S. Dual energy subtraction and temporal subtraction chest radiography. J Thorac Imaging. 2008;23:77–85. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
