

Accelerating regional atrophy rates in the progression from normal aging to Alzheimer's disease
- PMID: 19618189
- PMCID: PMC2778773
- DOI: 10.1007/s00330-009-1512-5
Accelerating regional atrophy rates in the progression from normal aging to Alzheimer's disease
Abstract
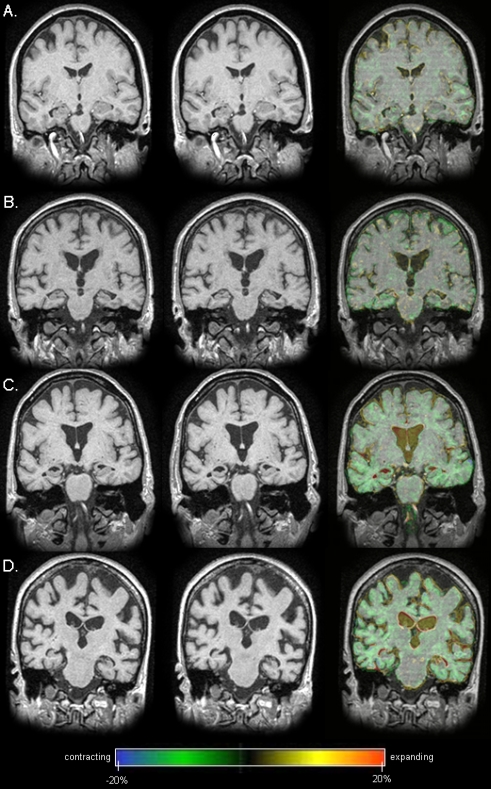
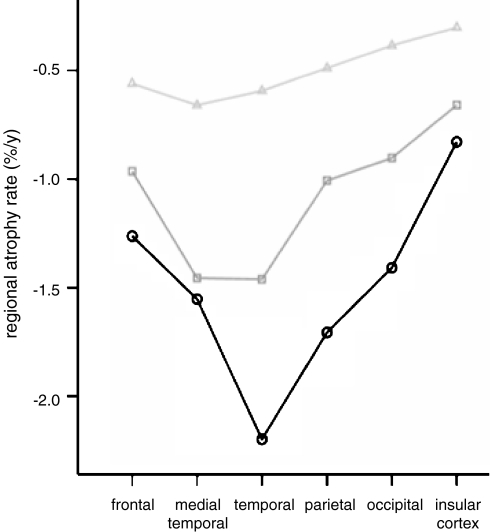
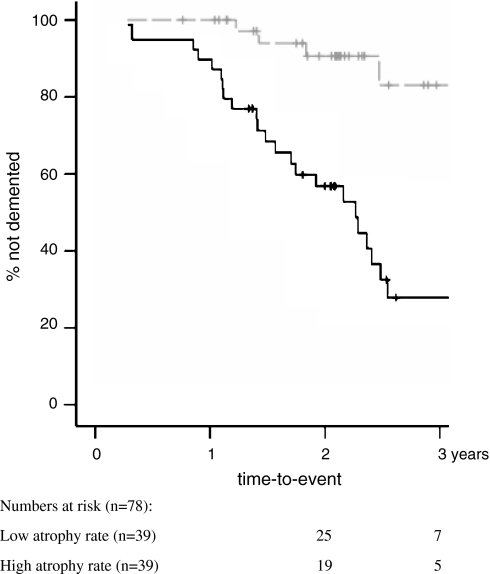
We investigated progression of atrophy in vivo, in Alzheimer's disease (AD), and mild cognitive impairment (MCI). We included 64 patients with AD, 44 with MCI and 34 controls with serial MRI examinations (interval 1.8 ± 0.7 years). A nonlinear registration algorithm (fluid) was used to calculate atrophy rates in six regions: frontal, medial temporal, temporal (extramedial), parietal, occipital lobes and insular cortex. In MCI, the highest atrophy rate was observed in the medial temporal lobe, comparable with AD. AD patients showed even higher atrophy rates in the extramedial temporal lobe. Additionally, atrophy rates in frontal, parietal and occipital lobes were increased. Cox proportional hazard models showed that all regional atrophy rates predicted conversion to AD. Hazard ratios varied between 2.6 (95% confidence interval (CI) = 1.1-6.2) for occipital atrophy and 15.8 (95% CI = 3.5-71.8) for medial temporal lobe atrophy. In conclusion, atrophy spreads through the brain with development of AD. MCI is marked by temporal lobe atrophy. In AD, atrophy rate in the extramedial temporal lobe was even higher. Moreover, atrophy rates also accelerated in parietal, frontal, insular and occipital lobes. Finally, in nondemented elderly, medial temporal lobe atrophy was most predictive of progression to AD, demonstrating the involvement of this region in the development of AD.
Figures
References
-
- Fox NC, Scahill RI, Crum WR, et al. Correlation between rates of brain atrophy and cognitive decline in AD. Neurology. 1999;52:1687–9. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
