

A cardiologic approach to non-insulin antidiabetic pharmacotherapy in patients with heart disease
- PMID: 19619327
- PMCID: PMC2723076
- DOI: 10.1186/1475-2840-8-38
A cardiologic approach to non-insulin antidiabetic pharmacotherapy in patients with heart disease
Abstract
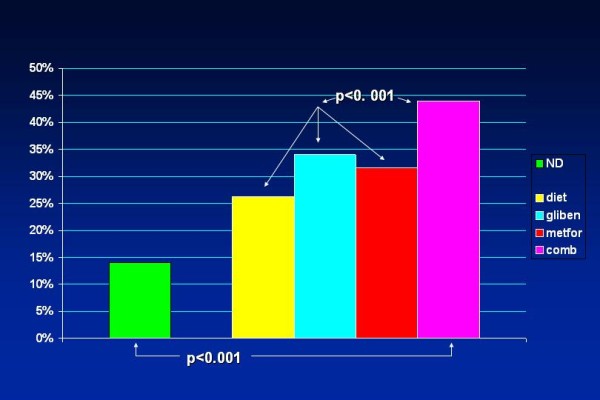
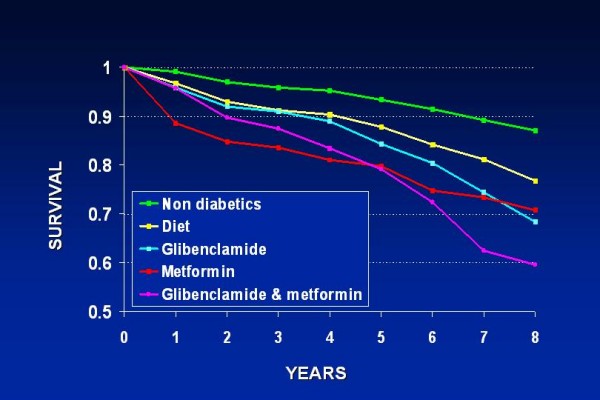
Classical non-insulin antihyperglycemic drugs currently approved for the treatment of type 2 diabetes mellitus (T2DM) comprise five groups: biguanides, sulfonylureas, meglitinides, glitazones and alpha-glucosidase inhibitors. Novel compounds are represented by the incretin mimetic drugs like glucagon like peptide-1 (GLP-1), the dipeptidyl peptidase 4 (DPP-4) inhibitors, dual peroxisome proliferator-activated receptors (PPAR) agonists (glitazars) and amylin mimetic drugs. We review the cardiovascular effects of these drugs in an attempt to improve knowledge regarding their potential risks when treating T2DM in cardiac patients. Metformin may lead to lethal lactic acidosis, especially in patients with clinical conditions that predispose to this complication, such as recent myocardial infarction, heart or renal failure. Sulfonylureas exert their effect by closing the ATP-dependent potassium channels. This prevents the opening of these channels during myocardial ischemia, impeding the necessary hyperpolarization that protects the cell. The combined sulfonylurea/metformin therapy reveals additive effects on mortality in patients with coronary artery disease (CAD). Meglitinides effects are similar to those of sulfonylureas, due to their almost analogous mechanism of action. Glitazones lower leptin levels, leading to weight gain and are unsafe in NYHA class III or IV. The long-term effects of alpha-glucosidase inhibitors on morbidity and mortality rates is yet unknown. The incretin GLP-1 is associated with reductions in body weight and appears to present positive inotropic effects. DPP-4 inhibitors influences on the cardiovascular system seem to be neutral and patients do not gain weight. The future of glitazars is presently uncertain following concerns about their safety. The amylin mimetic drug paramlintide, while a satisfactory adjuvant medication in insulin-dependent diabetes, is unlikely to play a major role in the management of T2DM. Summarizing the present information it can be stated that 1. Four out the five classical oral antidiabetic drug groups present proven or potential cardiac hazards; 2. These hazards are not mere 'side effects', but biochemical phenomena which are deeply rooted in the drugs' mechanism of action; 3. Current data indicate that the combined glibenclamide/metformin therapy seems to present special risk and should be avoided in the long-term management of T2DM with proven CAD; 4. Glitazones should be avoided in patients with overt heart failure; 5, The novel incretin mimetic drugs and DPP-4 inhibitors--while usually inadequate as monotherapy--appear to be satisfactory adjuvant drugs due to the lack of known undesirable cardiovascular effects; 6. Customized antihyperglycemic pharmacological approaches should be implemented for the achievement of optimal treatment of T2DM patients with heart disease. In this context, it should be carefully taken into consideration whether the leading clinical status is CAD or heart failure.
Figures
Similar articles
-
Non-insulin antidiabetic therapy in cardiac patients: current problems and future prospects.Adv Cardiol. 2008;45:154-170. doi: 10.1159/000115193. Adv Cardiol. 2008. PMID: 18230961 Review.
-
Oral antidiabetic therapy in patients with heart disease. A cardiologic standpoint.Herz. 2004 May;29(3):290-8. doi: 10.1007/s00059-004-2476-5. Herz. 2004. PMID: 15167955 Review.
-
Clinical pharmacology of antidiabetic drugs: What can be expected of their use?Presse Med. 2023 Mar;52(1):104158. doi: 10.1016/j.lpm.2022.104158. Epub 2022 Dec 22. Presse Med. 2023. PMID: 36565754
-
New drugs for type 2 diabetes mellitus: what is their place in therapy?Drugs. 2008;68(15):2131-62. doi: 10.2165/00003495-200868150-00005. Drugs. 2008. PMID: 18840004 Review.
-
Oral antidiabetic agents: current role in type 2 diabetes mellitus.Drugs. 2005;65(3):385-411. doi: 10.2165/00003495-200565030-00005. Drugs. 2005. PMID: 15669880 Review.
Cited by
-
Diabetic cardiomyopathy: signaling defects and therapeutic approaches.Expert Rev Cardiovasc Ther. 2010 Mar;8(3):373-91. doi: 10.1586/erc.10.17. Expert Rev Cardiovasc Ther. 2010. PMID: 20222816 Free PMC article. Review.
-
The C161T polymorphism in the peroxisome proliferator-activated receptor gamma gene (PPARγ) is associated with risk of coronary artery disease: a meta-analysis.Mol Biol Rep. 2013 Apr;40(4):3101-12. doi: 10.1007/s11033-012-2384-3. Epub 2012 Dec 25. Mol Biol Rep. 2013. PMID: 23266668
-
Activation of EGFR/ERBB2 via pathways involving ERK1/2, P38 MAPK, AKT and FOXO enhances recovery of diabetic hearts from ischemia-reperfusion injury.PLoS One. 2012;7(6):e39066. doi: 10.1371/journal.pone.0039066. Epub 2012 Jun 13. PLoS One. 2012. PMID: 22720029 Free PMC article.
-
The Pro12Ala polymorphism in the peroxisome proliferator-activated receptor gamma-2 gene (PPARγ2) is associated with increased risk of coronary artery disease: a meta-analysis.PLoS One. 2012;7(12):e53105. doi: 10.1371/journal.pone.0053105. Epub 2012 Dec 31. PLoS One. 2012. PMID: 23300871 Free PMC article.
-
Incretins as a novel therapeutic strategy in patients with diabetes and heart failure.Heart Fail Rev. 2013 Mar;18(2):141-8. doi: 10.1007/s10741-012-9318-y. Heart Fail Rev. 2013. PMID: 22570104 Review.
References
-
- Inzucchi SE, Sherwin RS. The prevention of type 2 diabetes mellitus. Endocrinol Metab Clin North Am. 2005;34:199–219. - PubMed
-
- Meinert CL, Knatterud GL, Prout TE, Klimt CR. A study of the effects of hypoglycemic agents on vascular complications in patients with adult-onset diabetes. II. Mortality results. Diabetes. 1970;19:789–830. - PubMed
-
- Smits P, Thien T. Cardiovascular effects of sulphonylurea derivatives. Implication for the treatment of NIDDM? Diabetologia. 1995;38:116–121. - PubMed
-
- Brady PA, Terzic A. The sulfonylurea controversy: more questions from the heart. J Am Coll Cardiol. 1998;31:950–956. - PubMed
-
- Innerfield RJ. Metformin-associated mortality in U.S. studies. N Engl J Med. 1996;334:1611–1613. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
