

Mitral valve hemodynamics after repair of acute posterior leaflet prolapse: quadrangular resection versus triangular resection versus neochordoplasty
- PMID: 19619772
- PMCID: PMC4375960
- DOI: 10.1016/j.jtcvs.2009.01.031
Mitral valve hemodynamics after repair of acute posterior leaflet prolapse: quadrangular resection versus triangular resection versus neochordoplasty
Abstract
Objective: Leaflet prolapse resulting from acute chordal rupture is one presentation of fibroelastic deficiency that is associated with minimal leaflet changes in the prolapsing segment. Minimizing resection and preserving leaflet tissue may be an optimal surgical strategy. We examined the importance of the leaflet preservation concept by comparing resective and nonresective surgical procedures in practice today.
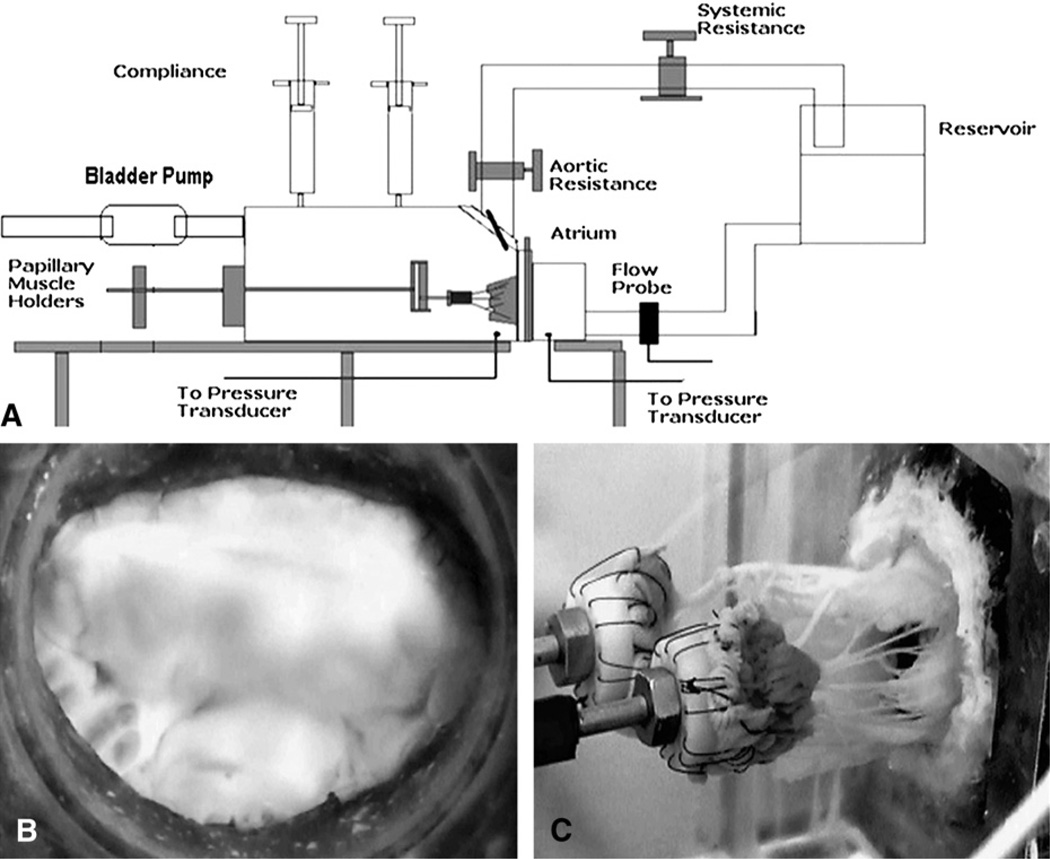
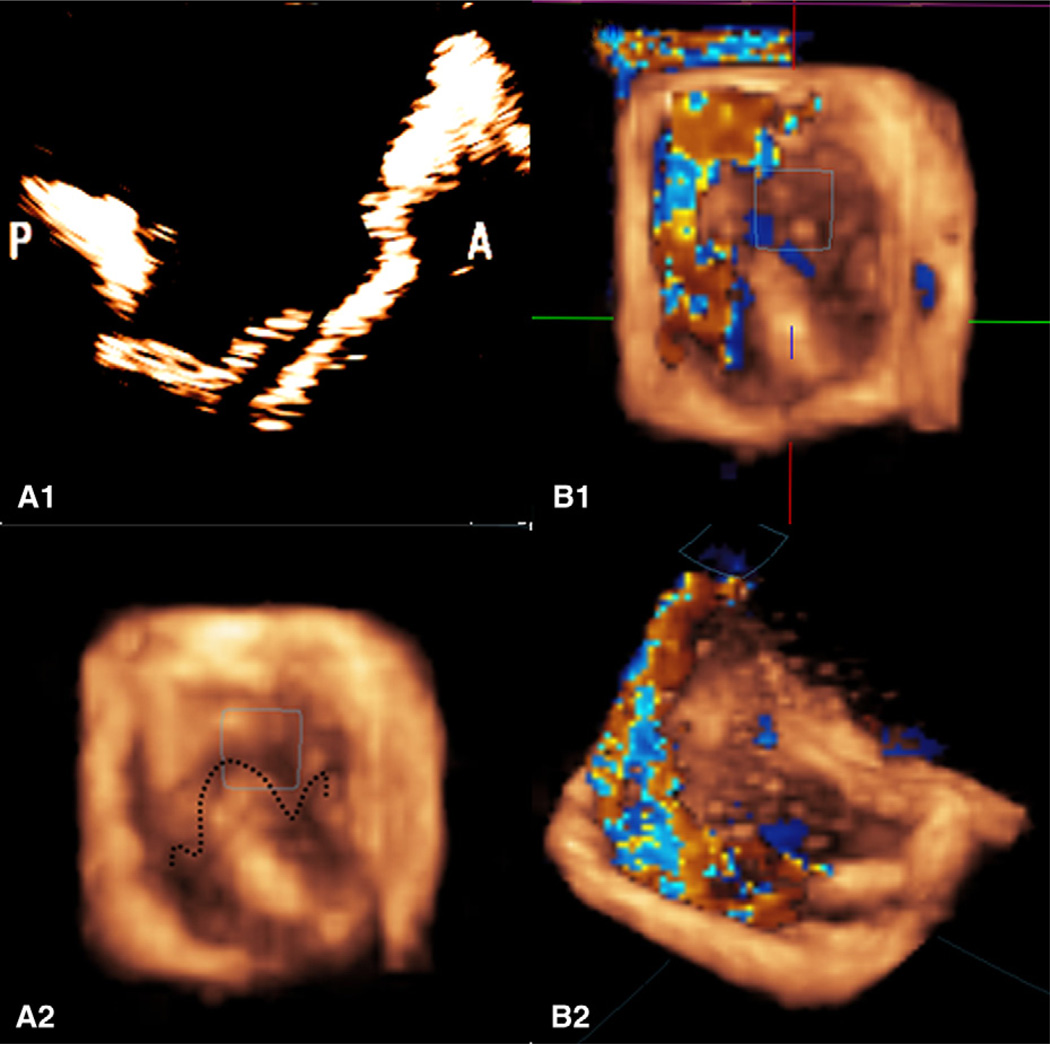
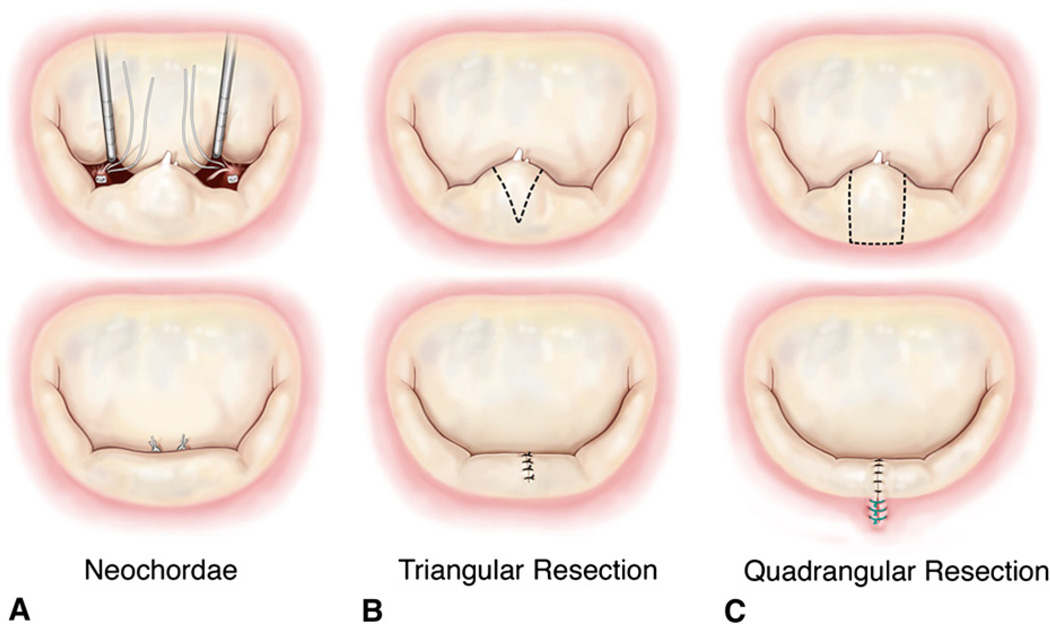
Methods: Eight porcine mitral valves were evaluated in an in vitro heart simulator before surgical manipulation. Mitral regurgitation was created in these valves by transecting the posterior marginal chordae resulting in severe P2 prolapse. After confirmation of mitral regurgiation via regurgitant flow measurement (mL/beat), regurgitation was corrected by three repairs: neochordoplasty with polytetrafluoroethylene sutures (Gore-Tex; W. L. Gore & Associates, Inc, Flagstaff, Ariz), triangular resection, and quadrangular resection with annular compression. Postrepair valve hemodynamics were quantified under pulsatile conditions of 120 mm Hg peak transmitral pressure and 5 L/min cardiac output at 70 beats/min. Furthermore, hemodynamic, geometric, and echocardiographic indices were measured.
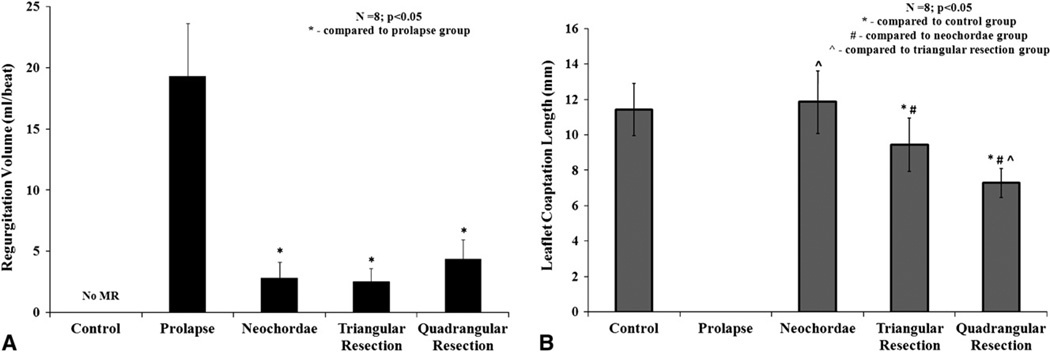
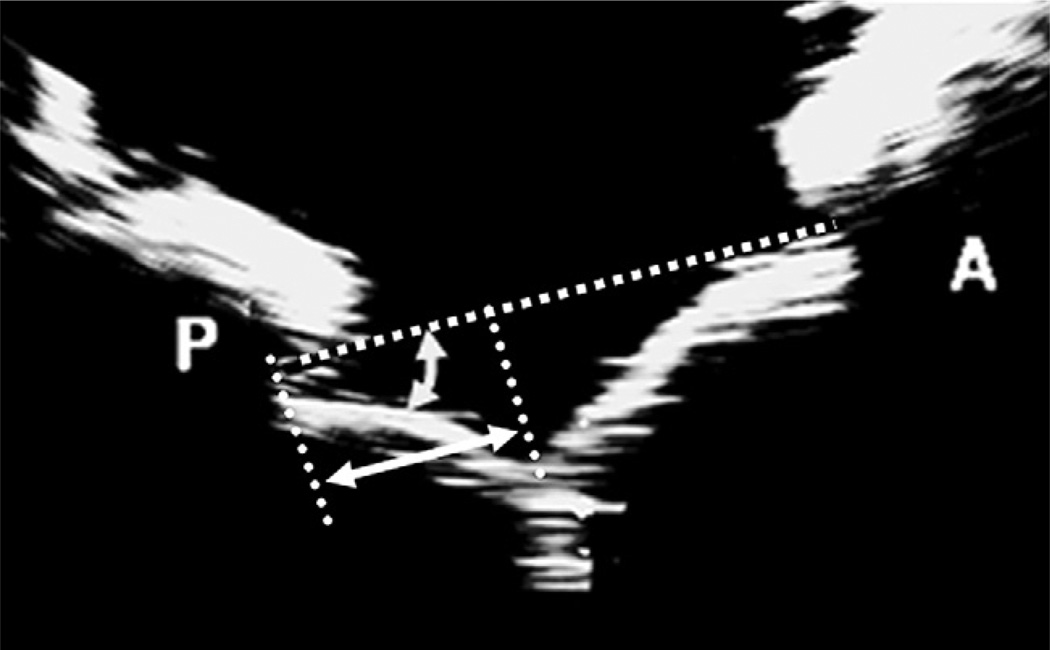
Results: Transecting the marginal chordae resulted in severe P2 prolapse and significant mitral regurgiation (19.3 +/- 4.3 mL/beat). Regurgitant volume was significantly reduced after any of the three surgical approaches (quadrangular, 4.38 +/- 1.6 mL/beat; triangular, 2.56 +/- 1.0 mL/beat; neochordal, 2.86 +/- 1.24 mL/beat). In comparison with the baseline normal valves, leaflet coaptation length and posterior leaflet mobility were significantly reduced in the quadrangular resection group, whereas they were partially restored in the triangular resection and fully preserved in the neochordoplasty group.
Conclusions: Although the three repair procedures are hemodynamically comparable, valve function and leaflet kinematics were significantly better after a nonresection or limited resective correction of leaflet prolapse in this experimental model of acute chordal rupture with otherwise normal leaflet geometry.
Figures
References
-
- Carpentier A. Cardiac valve surgery—the “French correction.”. J Thorac Cardiovasc Surg. 1983;86:323–337. - PubMed
-
- Anyanwu AC, Adams DH. Etiologic classification of degenerative mitral valve disease: Barlow’s disease and fibroelastic deficiency. Semin Thorac Cardiovasc Surg. 2007;19:90–96. - PubMed
-
- Fornes P, Heudes D, Fuzellier JF, Tixier D, Bruneval P, Carpentier A. Correlation between clinical and histologic patterns of degenerative mitral valve insufficiency: a histomorphometric study of 130 excised segments. Cardiovasc Pathol. 1999;8:81–92. - PubMed
-
- He S, Fontaine AA, Schwammenthal E, Yoganathan AP, Levine RA. Integrated mechanism for functional mitral regurgitation: leaflet restriction versus coapting force: in vitro studies. Circulation. 1997;96:1826–1834. - PubMed
-
- Jimenez JH, Liou SW, Padala M, He Z, Sacks M, Gorman RC, et al. A saddle-shaped annulus reduces systolic strain on the central region of the mitral valve anterior leaflet. J Thorac Cardiovasc Surg. 2007;134:1562–1568. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
