

Body mass index: surgical site infections and mortality after lower extremity bypass from the National Surgical Quality Improvement Program 2005-2007
- PMID: 19619975
- PMCID: PMC2817998
- DOI: 10.1016/j.avsg.2009.05.003
Body mass index: surgical site infections and mortality after lower extremity bypass from the National Surgical Quality Improvement Program 2005-2007
Abstract
Background: Patients undergoing lower extremity bypass are at high risk for surgical site infections (SSI). We examined lower extremity bypasses by graft origin and body mass index (BMI) classification to analyze differences in postoperative mortality and SSI occurrence.
Methods: The 2005-2007 National Surgical Quality Improvement Program (NSQIP), a multi-institutional risk-adjusted database, was queried to compare perioperative mortality (30-day), overall morbidity, and SSIs after lower extremity arterial bypass for peripheral arterial disease. Bypass was stratified by graft origin as aortoiliac, femoral, or popliteal. Patient demographics, comorbidities, operative, and postoperative occurrences were analyzed.
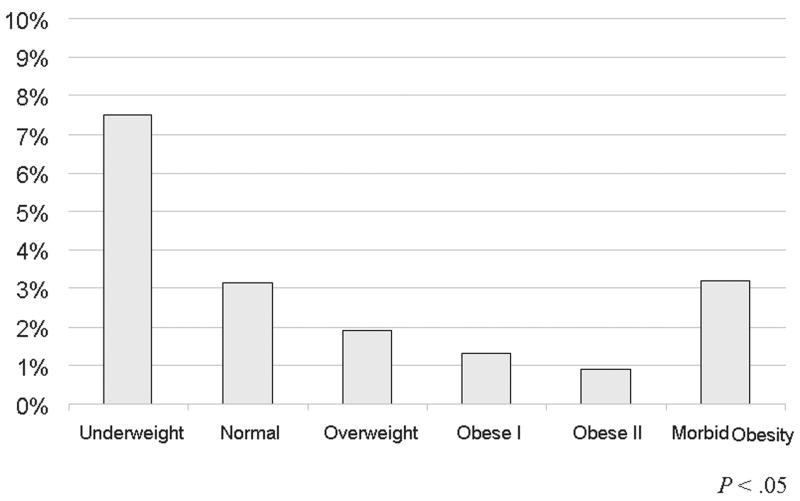
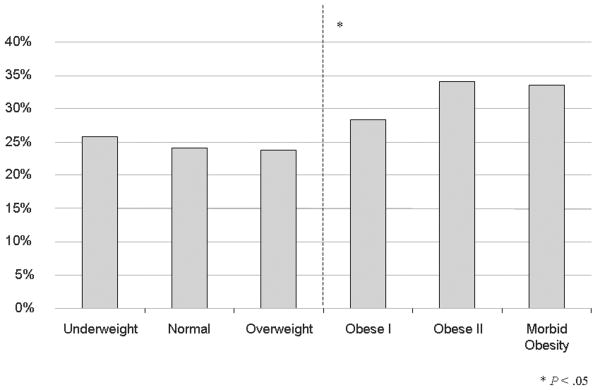
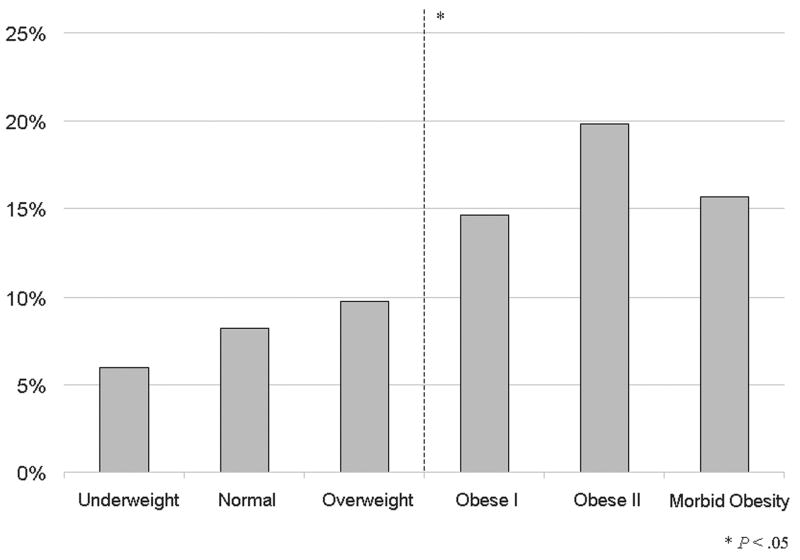
Results: There were 7,595 bypasses performed (1,596 aortoiliac, 5,483 femoral, and 516 popliteal). Mortality was similar regardless of bypass origin (2.8%, 2.4%, and 2.7%; p = 0.57). SSIs occurred in 11% of overall cases (10%, 11%, and 11%; p = 0.47). Graft failure was significantly associated with postoperative SSI occurrence (odds ratio [OR] = 2.4, 95% confidence interval [CI] 1.9-3.1, p < 0.001), as was postoperative sepsis (OR = 6.5, 95% CI 5.1-8.3, p < 0.001). Independent predictors of mortality were age, aortoiliac bypass origin, underweight, normal weight, morbid obesity (compared to overweight and obese), end-stage renal disease, poor preoperative functional status, preoperative sepsis, chronic obstructive pulmonary disease, hypoalbuminemia, and cardiac disease. Independent predictors of SSI were obesity, diabetes, poor preoperative functional status, a history of smoking, and female gender.
Conclusion: SSIs occur frequently after lower extremity bypass regardless of bypass origin and are associated with early graft failure and sepsis. Obesity predicts postoperative SSI. Mortality risk was greatest in the underweight, followed by morbidly obese and normal-weight patients, while overweight and mild to moderate obesity were associated with the lowest mortality.
Copyright 2010 Annals of Vascular Surgery Inc. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Blood transfusion is associated with increased morbidity and mortality after lower extremity revascularization.J Vasc Surg. 2010 Mar;51(3):616-21, 621.e1-3. doi: 10.1016/j.jvs.2009.10.045. Epub 2010 Jan 27. J Vasc Surg. 2010. PMID: 20110154
-
Predictors of surgical site infection after open lower extremity revascularization.J Vasc Surg. 2011 Aug;54(2):433-9. doi: 10.1016/j.jvs.2011.01.034. Epub 2011 Mar 31. J Vasc Surg. 2011. PMID: 21458203
-
Fewer Complications in the Obese Following Lower Extremity Endovascular Interventions.Ann Vasc Surg. 2018 May;49:17-23. doi: 10.1016/j.avsg.2017.10.030. Epub 2018 Feb 6. Ann Vasc Surg. 2018. PMID: 29421418 Free PMC article.
-
Factors associated with surgical site infection after lower extremity bypass in the Society for Vascular Surgery (SVS) Vascular Quality Initiative (VQI).J Vasc Surg. 2014 Nov;60(5):1238-1246. doi: 10.1016/j.jvs.2014.05.012. Epub 2014 Jun 20. J Vasc Surg. 2014. PMID: 24953898
-
Risk Factors for Surgical Site Infection after Lower Limb Revascularisation Surgery: a Systematic Review and Meta-Analysis of Prognostic Studies.Eur J Vasc Endovasc Surg. 2024 Mar;67(3):455-467. doi: 10.1016/j.ejvs.2023.10.038. Epub 2023 Nov 2. Eur J Vasc Endovasc Surg. 2024. PMID: 37925099
Cited by
-
Revascularisation through the obturator foramen of lower limbs with a compromised ipsilateral groin due to infection.Ann R Coll Surg Engl. 2020 Jan;102(1):14-17. doi: 10.1308/rcsann.2019.0070. Epub 2019 Jun 3. Ann R Coll Surg Engl. 2020. PMID: 31155915 Free PMC article.
-
The BMI Paradox and Robotic Assisted Partial Nephrectomy.Front Surg. 2020 Jan 9;6:74. doi: 10.3389/fsurg.2019.00074. eCollection 2019. Front Surg. 2020. PMID: 31998743 Free PMC article.
-
Surgical site infections (SSIs) after stoma reversal (SR): risk factors, implications, and protective strategies.J Gastrointest Surg. 2015 Feb;19(2):327-34. doi: 10.1007/s11605-014-2649-3. Epub 2014 Sep 13. J Gastrointest Surg. 2015. PMID: 25217092
-
Effects of the morbid obesity and skin incision choices on surgical outcomes in patients undergoing total abdominal hysterectomy.Turk J Obstet Gynecol. 2016 Dec;13(4):189-195. doi: 10.4274/tjod.67864. Epub 2016 Dec 15. Turk J Obstet Gynecol. 2016. PMID: 28913120 Free PMC article.
-
Prosthetic graft infections involving the femoral artery.J Vasc Surg. 2013 Mar;57(3):700-5. doi: 10.1016/j.jvs.2012.09.049. Epub 2013 Jan 9. J Vasc Surg. 2013. PMID: 23312940 Free PMC article.
References
-
- Nationwide (States, DC, and Territories)- 2007. Behavioral Risk Factor Surveillance System Survey Data. Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2007. Overweight and obesity. Centers for Disease Control and Prevention (CDC)
-
- Mullen JT, Davenport DL, Hutter MM, Hosokawa PW, Henderson WG, Khuri SF, et al. Impact of body mass index on perioperative outcomes in patients undergoing major intra-abdominal cancer surgery. Ann Surg Onc. 2008;15:2164–72. - PubMed
-
- Patel VI, Hamdan AD, Schermerhorn ML, Hile C, Dahlberg S, Campbell DR, et al. Lower extremity arterial revascularization in obese patients. J Vasc Surg. 2007;46:738–42. - PubMed
-
- Kent KC, Bartek S, Kuntz KM, Anninos E, Skillman JJ. Prospective study of wound complications in continuous infrainguinal incisions after lower limb arterial reconstruction: incidence, risk factors, and cost. Surgery. 1996;119:378–83. - PubMed
-
- Chang JK, Calligaro KD, Ryan S, Runyan D, Dougherty MJ, Stern JJ. Risk factors associated with infection of lower extremity revascularization: analysis of 365 procedures performed at a teaching hospital. Ann Vasc Surg. 2003;17:91–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
