

Pancreatic ductal adenocarcinoma with intratumoral cystic lesions on MRI: correlation with histopathological findings
- PMID: 19620175
- PMCID: PMC3473450
- DOI: 10.1259/bjr/69770140
Pancreatic ductal adenocarcinoma with intratumoral cystic lesions on MRI: correlation with histopathological findings
Abstract
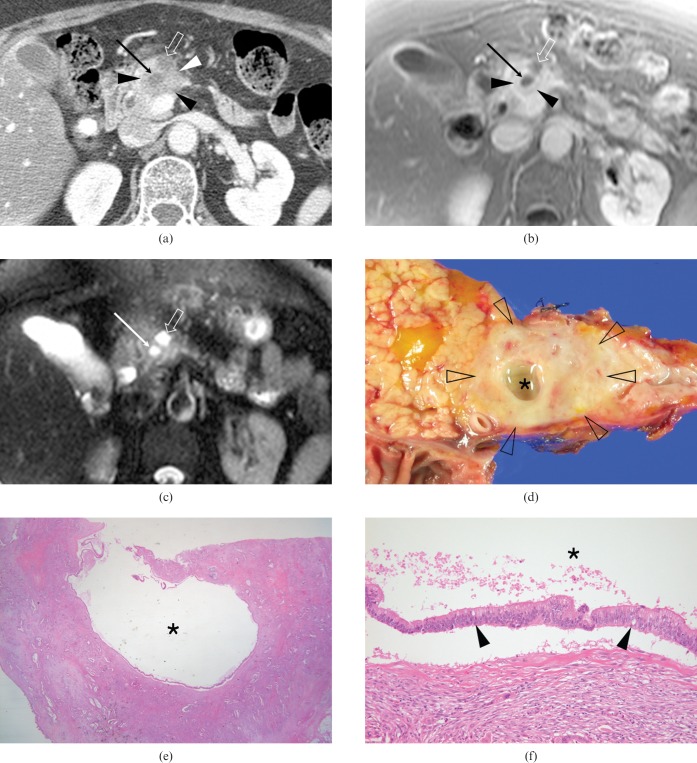
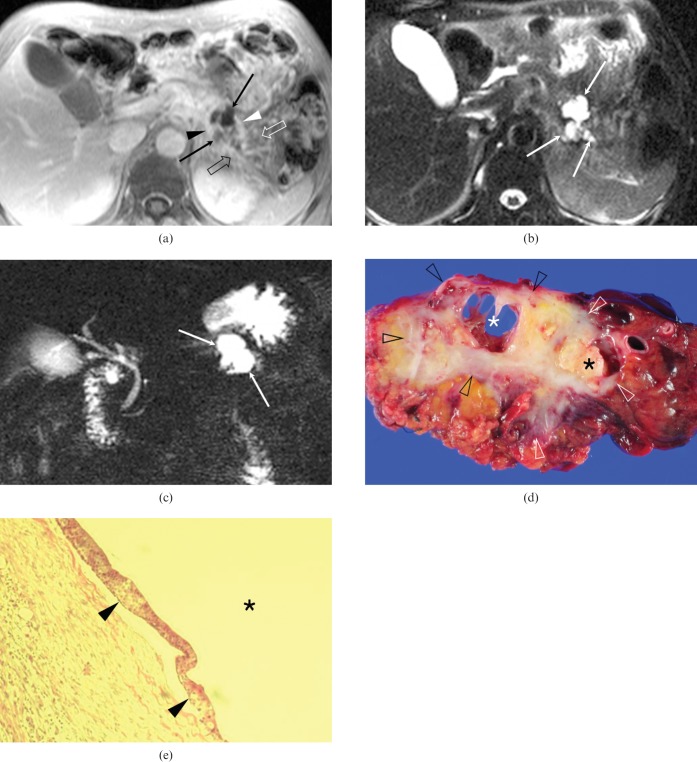
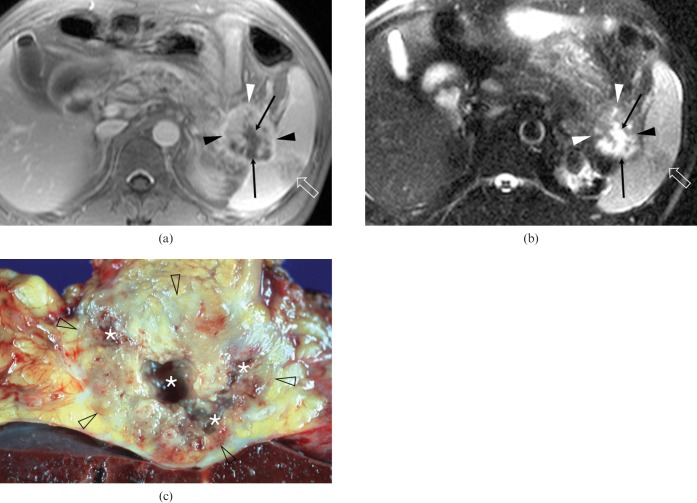
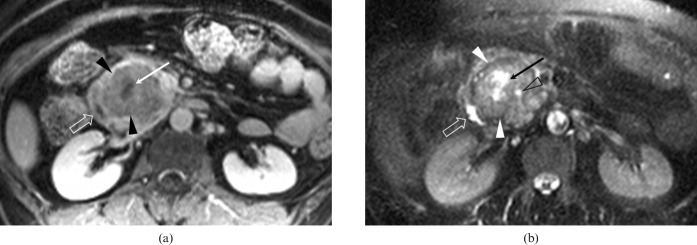
The purpose of this study was to evaluate intratumoral cystic lesions of pancreatic ductal adenocarcinoma (PDAC) depicted on MRI, and to correlate these cystic lesions with their histopathological findings. This study included 12 patients (7 males and 5 females; mean age, 59 years) with intratumoral cystic lesions of PDAC detected on a retrospective MRI review. We reviewed the histopathological findings of the cystic lesions within PDACs and analysed the MRI findings, focusing on the appearance of the intratumoral cystic lesions, i.e. the size, number, margin and intratumoral location, and on the ancillary findings of PDAC, i.e. peripancreatic infiltration, upstream pancreatic duct dilatation and distal parenchymal atrophy. Intratumoral cystic lesions were classified as neoplastic mucin cysts (n = 7, 58%) or cystic necrosis (n = 5, 42%) according to the histopathological findings; they ranged in greatest dimension from 0.5 cm to 3.4 cm (mean, 1.7 cm). Seven patients had only one cystic lesion each, while the remaining five had multiple cystic lesions. Most of the neoplastic mucin cysts had smooth margins (n = 6, 86%) and eccentric locations (n = 6), whereas most cystic necroses had irregular margins (n = 4, 80%) and centric locations (n = 4). The most common ancillary findings of PDAC were peripancreatic infiltration, distal pancreatic atrophy and upstream pancreatic duct dilatation (92%, 75% and 58%, respectively). The intratumoral cystic lesions of PDACs on MRI were classified as either neoplastic mucin cysts with smooth margins and eccentric locations or cystic necroses with irregular margins and centric locations.
Figures
References
-
- Greenlee RT, Murray T, Bolden S, Wingo PA. Cancer statistics, 2000. CA Cancer J Clin 2000;50:7–33 - PubMed
-
- Evans DB, Abbruzzese JL, Rich TA. Cancer of the pancreas. In: Devita VT, Hellman S, Rosenberg SA, editors. Cancer: Principles and Practice of Oncology. 5th edn. Philadelphia, PA: Lippincott-Raven, 1997:1054–87
-
- Kosmahl M, Pauser U, Anlauf M, Kloppel G. Pancreatic ductal adenocarcinomas with cystic features: neither rare nor uniform. Mod Pathol 2005;18:1157–64 - PubMed
-
- Brugge WR, Lauwers GY, Sahani D, Fernandez-del Castillo C, Warshaw AL. Cystic neoplasms of the pancreas. N Engl J Med 2004;351:1218–26 - PubMed
-
- Gasslander T, Arnelo U, Albiin N, Permert J. Cystic tumors of the pancreas. Dig Dis 2001;19:57–62 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
