

Repair of acute myocardial infarction by human stemness factors induced pluripotent stem cells
- PMID: 19620500
- PMCID: PMC2768575
- DOI: 10.1161/CIRCULATIONAHA.109.865154
Repair of acute myocardial infarction by human stemness factors induced pluripotent stem cells
Abstract
Background: Nuclear reprogramming provides an emerging strategy to produce embryo-independent pluripotent stem cells from somatic tissue. Induced pluripotent stem cells (iPS) demonstrate aptitude for de novo cardiac differentiation, yet their potential for heart disease therapy has not been tested.
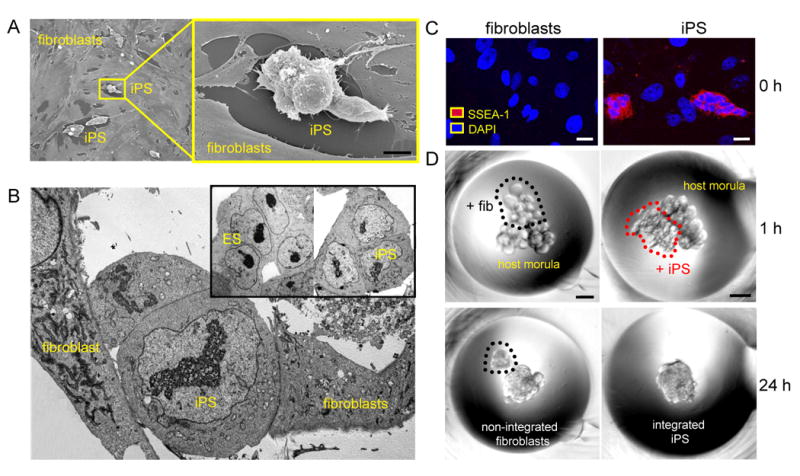
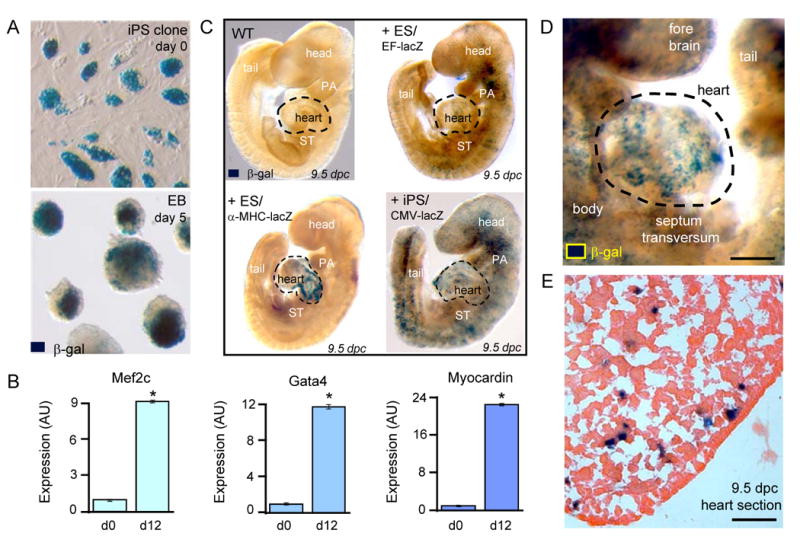
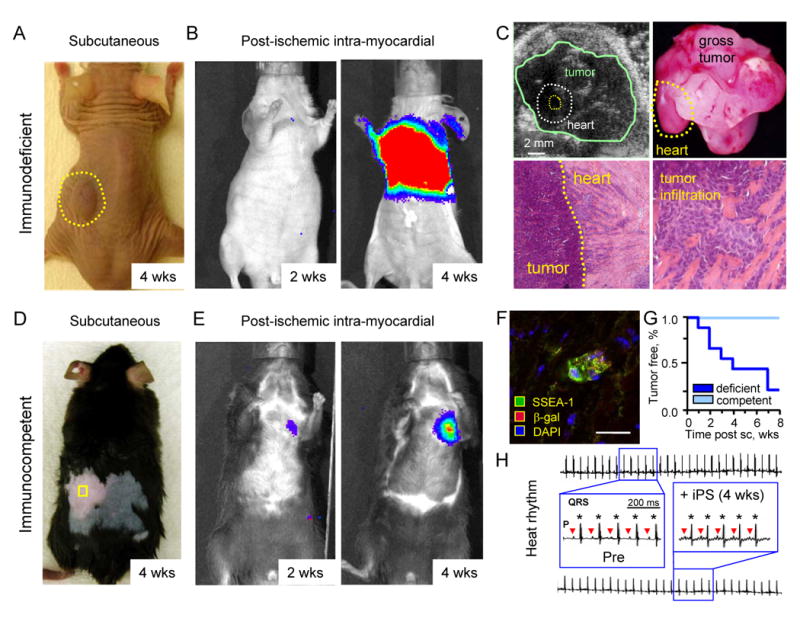
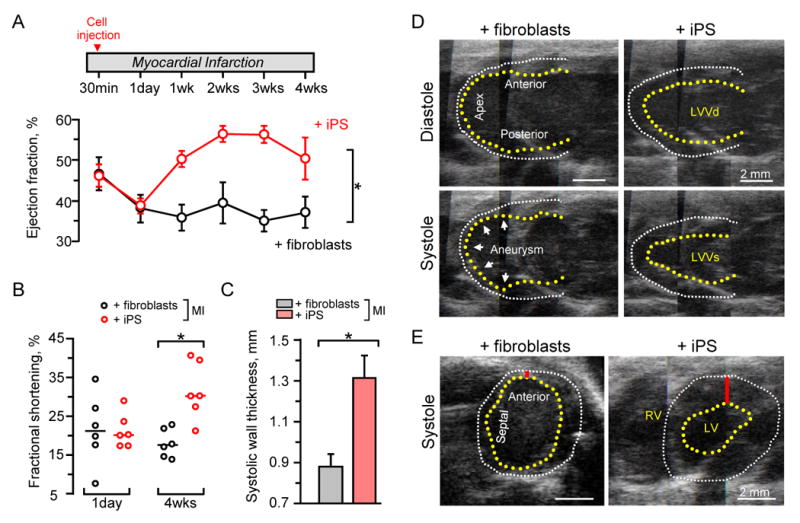
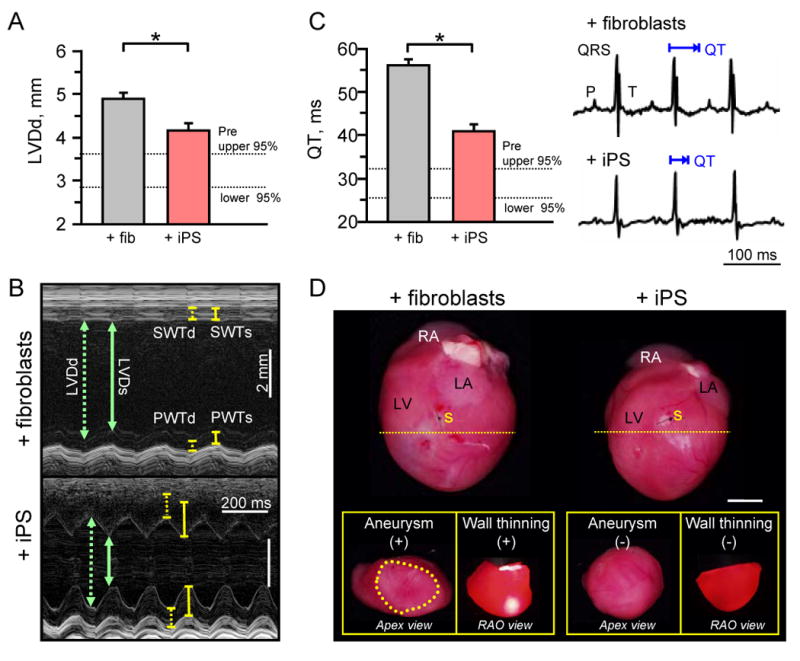
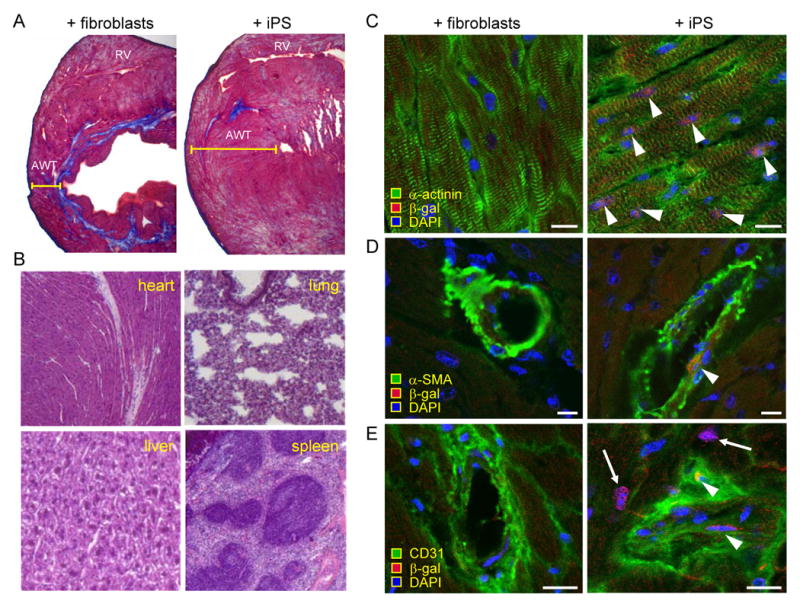
Methods and results: In this study, fibroblasts transduced with human stemness factors OCT3/4, SOX2, KLF4, and c-MYC converted into an embryonic stem cell-like phenotype and demonstrated the ability to spontaneously assimilate into preimplantation host morula via diploid aggregation, unique to bona fide pluripotent cells. In utero, iPS-derived chimera executed differentiation programs to construct normal heart parenchyma patterning. Within infarcted hearts in the adult, intramyocardial delivery of iPS yielded progeny that properly engrafted without disrupting cytoarchitecture in immunocompetent recipients. In contrast to parental nonreparative fibroblasts, iPS treatment restored postischemic contractile performance, ventricular wall thickness, and electric stability while achieving in situ regeneration of cardiac, smooth muscle, and endothelial tissue.
Conclusions: Fibroblasts reprogrammed by human stemness factors thus acquire the potential to repair acute myocardial infarction, establishing iPS in the treatment of heart disease.
Conflict of interest statement
Figures
References
-
- Daley GQ, Scadden DT. Prospects for stem cell-based therapy. Cell. 2008;132:544–548. - PubMed
-
- Segers V, Lee RT. Stem-cell therapy for cardiac disease. Nature. 2008;451:937–942. - PubMed
-
- Yamanaka S. Strategies and new developments in the generation of patient-specific pluripotent stem cells. Cell Stem Cell. 2007;1:39–49. - PubMed
-
- Nishikawa S, Goldstein RA, Nierras CR. The promise of human induced pluripotent stem cells for research and therapy. Nat Rev Mol Cell Biol. 2008;9:725–729. - PubMed
-
- Takahashi K, Okita K, Nakagawa M, Yamanaka S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell. 2006;126:663–676. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
