

Using dermoscopic criteria and patient-related factors for the management of pigmented melanocytic nevi
- PMID: 19620566
- PMCID: PMC2856040
- DOI: 10.1001/archdermatol.2009.115
Using dermoscopic criteria and patient-related factors for the management of pigmented melanocytic nevi
Abstract
Objective: To review recent dermoscopy studies that provide new insights into the evolution of nevi and their patterns of pigmentation as they contribute to the diagnosis of nevi and the management of pigmented melanocytic nevi.
Data sources: Data for this article were identified by searching the English and German literature by Medline and Journals@Ovid search for the period 1950 to January 2009.
Study selection: The following relevant terms were used: dermoscopy, dermatoscopy, epiluminescence microscopy (ELM), surface microscopy, digital dermoscopy, digital dermatoscopy, digital epiluminescence microscopy, digital surface microscopy, melanocytic skin lesion, nevi, and pigmented skin lesions. There were no exclusion criteria.
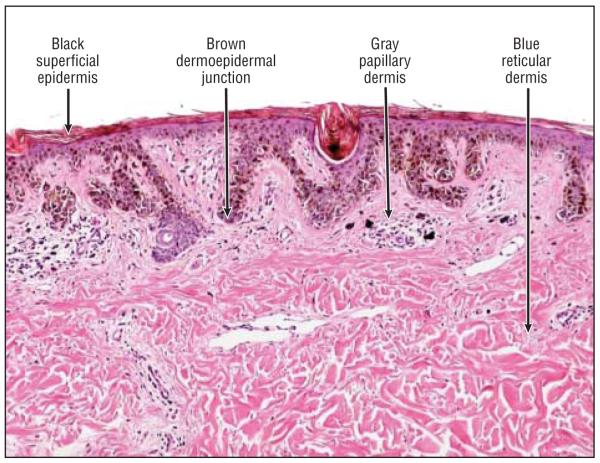
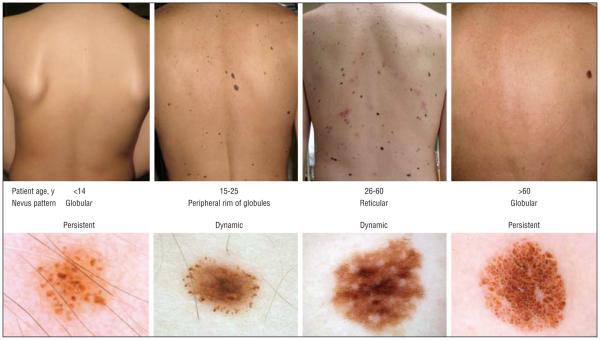
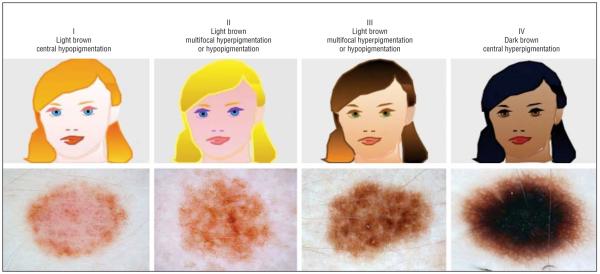
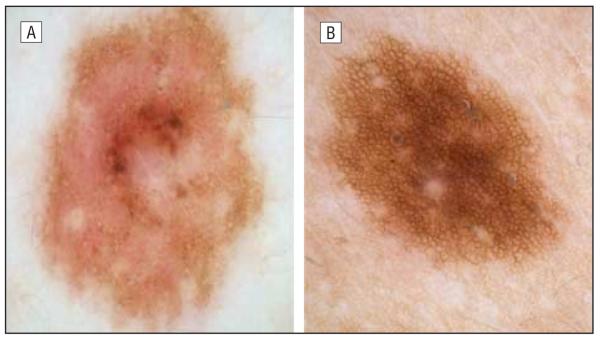
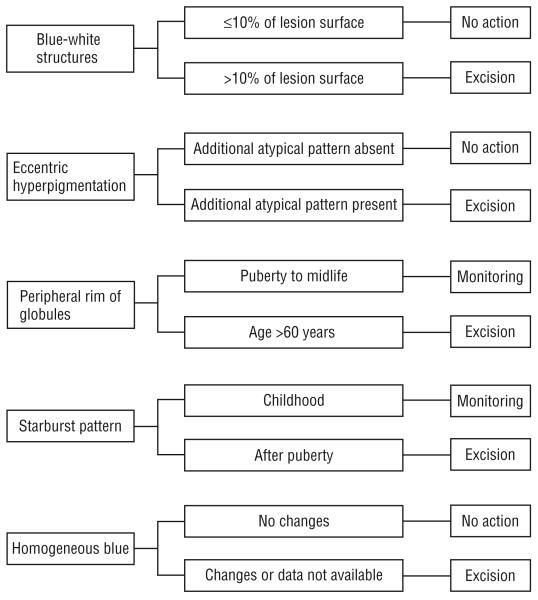
Data synthesis: The dermoscopic diagnosis of nevi relies on the following 4 criteria (each of which is characterized by 4 variables): (1) color (black, brown, gray, and blue); (2) pattern (globular, reticular, starburst, and homogeneous blue pattern); (3) pigment distribution (multifocal, central, eccentric, and uniform); and (4) special sites (face, acral areas, nail, and mucosa). In addition, the following 6 factors related to the patient might influence the pattern of pigmentation of the individual nevi: age, skin type, history of melanoma, UV exposure, pregnancy, and growth dynamics.
Conclusions: The 4 x 4 x 6 "rule" may help clinicians remember the basic dermoscopic criteria of nevi and the patient-related factors influencing their patterns. Dermoscopy is a useful technique for diagnosing melanocytic nevi, but the clinician should take additional factors into consideration to optimize the management of cases of pigmented lesions.
Figures



Similar articles
-
Dermoscopic patterns of 158 acral melanocytic nevi in a Latin American population.Actas Dermosifiliogr. 2013 Sep;104(7):586-92. doi: 10.1016/j.adengl.2013.01.002. Actas Dermosifiliogr. 2013. PMID: 23985085
-
Diagnostic significance of the blue hue in dermoscopy of melanocytic lesions: a dermoscopic-pathologic study.Am J Dermatopathol. 2001 Oct;23(5):463-9. doi: 10.1097/00000372-200110000-00013. Am J Dermatopathol. 2001. PMID: 11801781
-
[Dermoscopic pattern analysis of acral melanocytic nevi].Przegl Lek. 2013;70(11):911-5. Przegl Lek. 2013. PMID: 24697028 Polish.
-
Melanocytic nevi with special features: clinical-dermoscopic and reflectance confocal microscopic-findings.J Eur Acad Dermatol Venereol. 2014 Jul;28(7):833-45. doi: 10.1111/jdv.12291. Epub 2013 Oct 31. J Eur Acad Dermatol Venereol. 2014. PMID: 24171788 Review.
-
Role of In Vivo Reflectance Confocal Microscopy in the Analysis of Melanocytic Lesions.Acta Dermatovenerol Croat. 2018 Apr;26(1):64-67. Acta Dermatovenerol Croat. 2018. PMID: 29782304 Review.
Cited by
-
Artificial Intelligence in Dermatology: Challenges and Perspectives.Dermatol Ther (Heidelb). 2022 Dec;12(12):2637-2651. doi: 10.1007/s13555-022-00833-8. Epub 2022 Oct 28. Dermatol Ther (Heidelb). 2022. PMID: 36306100 Free PMC article.
-
The most common mistakes on dermatoscopy of melanocytic lesions.Postepy Dermatol Alergol. 2015 Feb;32(1):33-9. doi: 10.5114/pdia.2014.44029. Epub 2015 Feb 3. Postepy Dermatol Alergol. 2015. PMID: 25821425 Free PMC article. Review.
-
Malignant melanoma: epidemiologic aspects, diagnostic and therapeutic approach.Wien Med Wochenschr. 2013 Aug;163(15-16):354-8. doi: 10.1007/s10354-013-0207-3. Epub 2013 May 29. Wien Med Wochenschr. 2013. PMID: 23715934 Review.
-
Hemosiderotic dermatofibroma.An Bras Dermatol. 2017 Jan-Feb;92(1):92-94. doi: 10.1590/abd1806-4841.20173563. An Bras Dermatol. 2017. PMID: 28225963 Free PMC article.
-
Melanoma in Pregnancy-Diagnosis, Treatment, and Consequences for Fetal Development and the Maintenance of Pregnancy.Cancers (Basel). 2024 Jun 7;16(12):2173. doi: 10.3390/cancers16122173. Cancers (Basel). 2024. PMID: 38927879 Free PMC article. Review.
References
-
- Bystryn JC. Epiluminescence microscopy: a reevaluation of its purpose. Arch Dermatol. 2001;137(3):377–379. - PubMed
-
- Carli P, De Giorgi V, Crocetti E, et al. Improvement of malignant/benign ratio in excised melanocytic lesions in the “dermoscopy era”: a retrospective study 1997-2001. Br J Dermatol. 2004;150(4):687–692. - PubMed
-
- Gachon J, Beaulieu P, Sei JF, et al. First prospective study of the recognition process of melanoma in dermatological practice. Arch Dermatol. 2005;141(4):434–438. - PubMed
-
- Scope A, Dusza SW, Halpern AC, et al. The “ugly duckling” sign: agreement between observers. Arch Dermatol. 2008;144(1):58–64. - PubMed
-
- Hofmann-Wellenhof R, Blum A, Wolf IH, et al. Dermoscopic classification of atypical melanocytic nevi (Clark nevi) Arch Dermatol. 2001;137(12):1575–1580. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
