

Neural transplants in patients with Huntington's disease undergo disease-like neuronal degeneration
- PMID: 19620721
- PMCID: PMC2713393
- DOI: 10.1073/pnas.0904239106
Neural transplants in patients with Huntington's disease undergo disease-like neuronal degeneration
Abstract
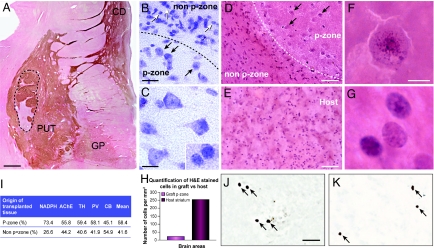
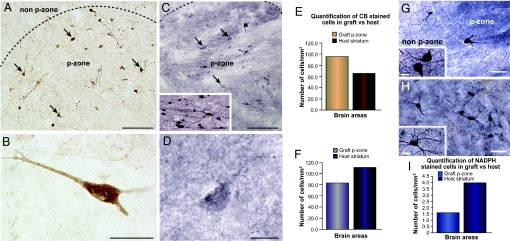
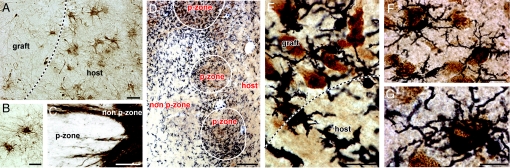
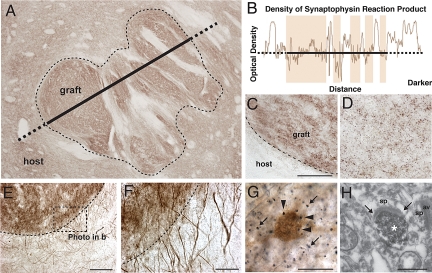
The clinical evaluation of neural transplantation as a potential treatment for Huntington's disease (HD) was initiated in an attempt to replace lost neurons and improve patient outcomes. Two of 3 patients with HD reported here, who underwent neural transplantation containing striatal anlagen in the striatum a decade earlier, have demonstrated marginal and transient clinical benefits. Their brains were evaluated immunohistochemically and with electron microscopy for markers of projection neurons and interneurons, inflammatory cells, abnormal huntingtin protein, and host-derived connectivity. Surviving grafts were identified bilaterally in 2 of the subjects and displayed classic striatal projection neurons and interneurons. Genetic markers of HD were not expressed within the graft. Here we report in patients with HD that (i) graft survival is attenuated long-term; (ii) grafts undergo disease-like neuronal degeneration with a preferential loss of projection neurons in comparison to interneurons; (iii) immunologically unrelated cells degenerate more rapidly than the patient's neurons, particularly the projection neuron subtype; (iv) graft survival is attenuated in the caudate in comparison to the putamen in HD; (v) glutamatergic cortical neurons project to transplanted striatal neurons; and (vi) microglial inflammatory changes in the grafts specifically target the neuronal components of the grafts. These results, when combined, raise uncertainty about this potential therapeutic approach for the treatment of HD. However, these observations provide new opportunities to investigate the underlying mechanisms involved in HD, as well as to explore additional therapeutic paradigms.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Comment in
-
No evidence for disease-like processes in fetal transplants.Proc Natl Acad Sci U S A. 2009 Sep 15;106(37):E104; author reply E105. doi: 10.1073/pnas.0908169106. Epub 2009 Sep 2. Proc Natl Acad Sci U S A. 2009. PMID: 19805203 Free PMC article. No abstract available.
Similar articles
-
Striatal parvalbuminergic neurons are lost in Huntington's disease: implications for dystonia.Mov Disord. 2013 Oct;28(12):1691-9. doi: 10.1002/mds.25624. Epub 2013 Sep 3. Mov Disord. 2013. PMID: 24014043 Free PMC article.
-
Histological findings on fetal striatal grafts in a Huntington's disease patient early after transplantation.Neuroscience. 2009 May 19;160(3):661-75. doi: 10.1016/j.neuroscience.2009.02.035. Epub 2009 Feb 28. Neuroscience. 2009. PMID: 19254752
-
Cellular localization of huntingtin in striatal and cortical neurons in rats: lack of correlation with neuronal vulnerability in Huntington's disease.J Neurosci. 1999 Feb 15;19(4):1189-202. doi: 10.1523/JNEUROSCI.19-04-01189.1999. J Neurosci. 1999. PMID: 9952397 Free PMC article.
-
Disrupted striatal neuron inputs and outputs in Huntington's disease.CNS Neurosci Ther. 2018 Apr;24(4):250-280. doi: 10.1111/cns.12844. CNS Neurosci Ther. 2018. PMID: 29582587 Free PMC article. Review.
-
Neuronal degeneration in striatal transplants and Huntington's disease: potential mechanisms and clinical implications.Brain. 2011 Mar;134(Pt 3):641-52. doi: 10.1093/brain/awq328. Epub 2011 Jan 28. Brain. 2011. PMID: 21278084 Review.
Cited by
-
Differential diagnosis of chorea.Curr Neurol Neurosci Rep. 2011 Aug;11(4):385-95. doi: 10.1007/s11910-011-0202-2. Curr Neurol Neurosci Rep. 2011. PMID: 21465146 Review.
-
Stem and Progenitor Cell-Based Therapy of the Central Nervous System: Hopes, Hype, and Wishful Thinking.Cell Stem Cell. 2016 Feb 4;18(2):174-88. doi: 10.1016/j.stem.2016.01.012. Cell Stem Cell. 2016. PMID: 26849304 Free PMC article. Review.
-
Abnormal morphology of peripheral cell tissues from patients with Huntington disease.J Neural Transm (Vienna). 2010 Jan;117(1):77-83. doi: 10.1007/s00702-009-0328-4. Epub 2009 Oct 16. J Neural Transm (Vienna). 2010. PMID: 19834779
-
Current understanding of the glial response to disorders of the aging CNS.Front Pharmacol. 2012 May 28;3:95. doi: 10.3389/fphar.2012.00095. eCollection 2012. Front Pharmacol. 2012. PMID: 22654755 Free PMC article.
-
Outcome of cell suspension allografts in a patient with Huntington's disease.Ann Neurol. 2018 Dec;84(6):950-956. doi: 10.1002/ana.25354. Epub 2018 Oct 25. Ann Neurol. 2018. PMID: 30286516 Free PMC article.
References
-
- Huntington's Disease Collaborative Research Group. A novel gene containing a trinucleotide repeat that is expanded and unstable on Huntington's disease chromosomes. Cell. 1993;72:971–983. - PubMed
-
- Freeman TB, Hauser RA, Sanberg PR, Saporta S. Neural transplantation for the treatment of Huntington's disease. Prog Brain Res. 2000;127:405–411. - PubMed
-
- Freeman TB, et al. Transplantation of human fetal striatal tissue in Huntington's disease: rationale for clinical studies. Neural transplantation in neurodegenerative disease: current status and new directions. Novartis Found Symp. 2000;231:129–144. - PubMed
-
- Peschanski M, Cesaro P, Hantraye P. Rationale for intrastriatal grafting of striatal neuroblasts in patients with Huntington's disease. Neuroscience. 1995;68:273–285. - PubMed
-
- Schmidt RH, Bjorklund A, Stenevi U. Intracerebral grafting of dissociated CNS tissue suspensions: a new approach for neuronal transplantation to deep brain sites. Brain Res. 1981;218:347–356. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
