

Acute stroke diagnosis
Abstract
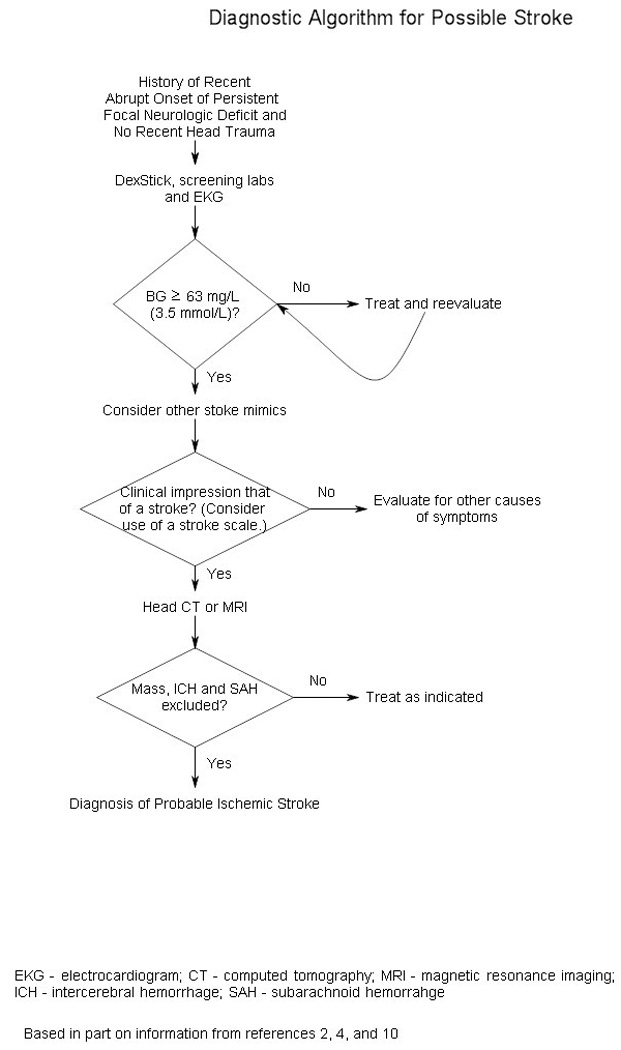
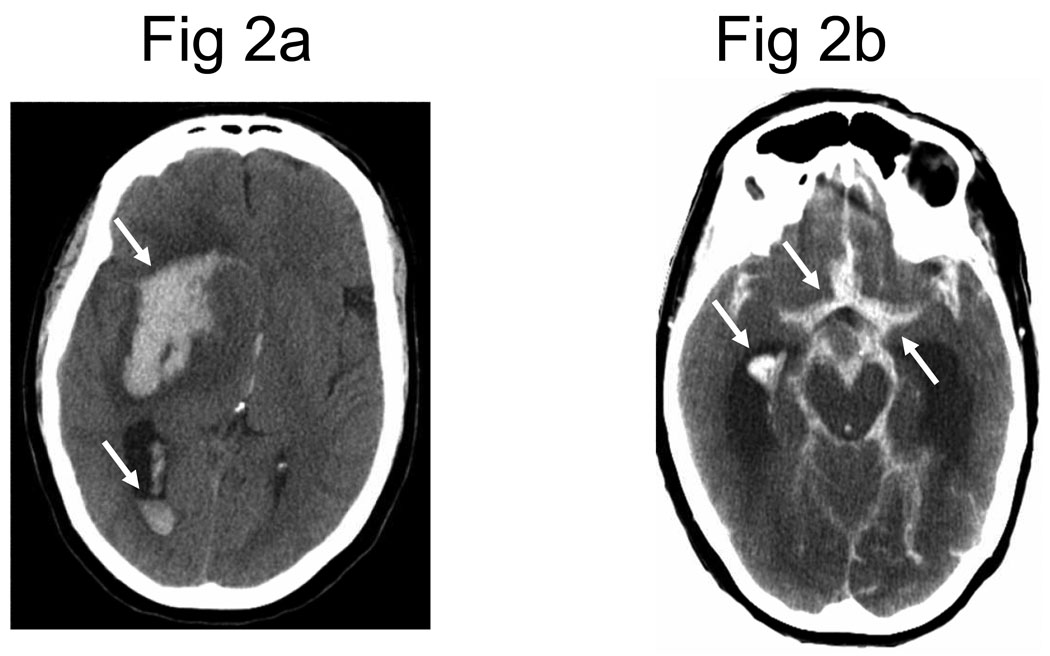
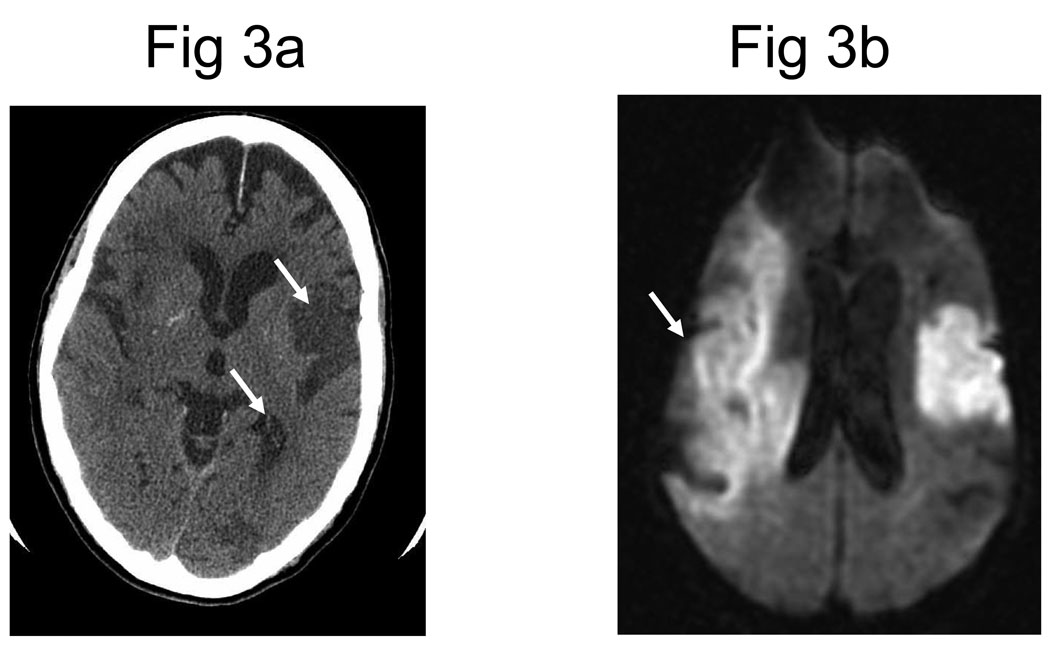
Stroke can be categorized as ischemic stroke, intracerebral hemorrhage, and subarachnoid hemorrhage. Awakening with or experiencing the abrupt onset of focal neurologic deficits is the hallmark of ischemic stroke diagnosis. The most common presenting symptoms for ischemic stroke are difficulty with speech and weakness on one half of the body. Many stroke mimics exist; two of the most common are a postictal seizure and hypoglycemia. Taking a detailed history and performing ancillary testing will usually exclude stroke mimics. Neuroimaging is required to differentiate ischemic stroke from intracerebral hemorrhage, as well as to diagnose entities other than stroke. The choice of neuroimaging depends on its availability, eligibility for acute stroke interventions, and the presence of patient contraindications. Subarachnoid hemorrhage presents most commonly with severe headache and may require analysis of cerebrospinal fluid when neuroimaging is not definitive. Public education of common presenting stroke symptoms is needed for patients to activate emergency medical services as soon as possible after the onset of stroke.
Figures
Similar articles
-
Diagnosis of acute stroke.Am Fam Physician. 2015 Apr 15;91(8):528-36. Am Fam Physician. 2015. PMID: 25884860 Review.
-
Can perfusion CT unmask postictal stroke mimics? A case-control study of 133 patients.Neurology. 2018 Nov 13;91(20):e1918-e1927. doi: 10.1212/WNL.0000000000006501. Epub 2018 Oct 17. Neurology. 2018. PMID: 30333164
-
Trial design and reporting standards for intra-arterial cerebral thrombolysis for acute ischemic stroke.Stroke. 2003 Aug;34(8):e109-37. doi: 10.1161/01.STR.0000082721.62796.09. Epub 2003 Jul 17. Stroke. 2003. PMID: 12869717
-
Should DWI MRI be the primary screening test for stroke?Int J Stroke. 2014 Aug;9(6):696-7. doi: 10.1111/ijs.12316. Int J Stroke. 2014. PMID: 25043518
-
Stroke Mimics and Acute Stroke Evaluation: Clinical Differentiation and Complications after Intravenous Tissue Plasminogen Activator.J Emerg Med. 2015 Aug;49(2):244-52. doi: 10.1016/j.jemermed.2014.12.072. Epub 2015 Mar 20. J Emerg Med. 2015. PMID: 25802155 Review.
Cited by
-
Role of autophagy in neurotoxic protein's clearance following post-ischemic stroke: where we are and what we know?Mol Brain. 2025 Jul 8;18(1):60. doi: 10.1186/s13041-025-01201-1. Mol Brain. 2025. PMID: 40629391 Free PMC article. Review.
-
Machine Learning for Medical Image Translation: A Systematic Review.Bioengineering (Basel). 2023 Sep 12;10(9):1078. doi: 10.3390/bioengineering10091078. Bioengineering (Basel). 2023. PMID: 37760180 Free PMC article. Review.
-
A two-level model for the analysis of syndrome of acute ischemic stroke: from diagnostic model to molecular mechanism.Evid Based Complement Alternat Med. 2013;2013:293010. doi: 10.1155/2013/293010. Epub 2013 Apr 4. Evid Based Complement Alternat Med. 2013. PMID: 23662126 Free PMC article.
-
Deep learning derived automated ASPECTS on non-contrast CT scans of acute ischemic stroke patients.Hum Brain Mapp. 2022 Jul;43(10):3023-3036. doi: 10.1002/hbm.25845. Epub 2022 Mar 31. Hum Brain Mapp. 2022. PMID: 35357053 Free PMC article.
-
Inflammatory, regulatory, and autophagy co-expression modules and hub genes underlie the peripheral immune response to human intracerebral hemorrhage.J Neuroinflammation. 2019 Mar 5;16(1):56. doi: 10.1186/s12974-019-1433-4. J Neuroinflammation. 2019. PMID: 30836997 Free PMC article.
References
-
- Rosamond W, Flegal K, Furie K, et al. Heart disease and stroke statistics–2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117(4):e25–e146. - PubMed
-
- Adams HP, Jr, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke. 1993;24(1):35–41. Medline. - PubMed
-
- Kumar S, Caplan LR. Why identification of stroke syndromes is still important. Curr Opin Neurol. 2007;20(1):78–82. Medline. - PubMed
-
- Hand PJ, Haisma JA, Kwan J, et al. Interobserver agreement for the bedside clinical assessment of suspected stroke. Stroke. 2006;37(3):776–780. Medline. - PubMed
-
- Kraaijeveld CL, van Gijn J, Schouten HJ, Staal A. Interobserver agreement for the diagnosis of transient ischemic attacks. Stroke. 1984;15(4):723–725. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
