

HIV subtype D is associated with dementia, compared with subtype A, in immunosuppressed individuals at risk of cognitive impairment in Kampala, Uganda
- PMID: 19622045
- PMCID: PMC2941149
- DOI: 10.1086/605284
HIV subtype D is associated with dementia, compared with subtype A, in immunosuppressed individuals at risk of cognitive impairment in Kampala, Uganda
Abstract
Background: In the United States, clade B is the predominant human immunodeficiency virus (HIV) subtype, whereas in sub-Saharan Africa, clades A, C, and D are the predominant subtypes. HIV subtype may have an impact on HIV disease progression. The effect of HIV subtype on the risk of dementia has, to our knowledge, not been examined. The objective of this study was to examine the relationship between HIV subtype and the severity of HIV-associated cognitive impairment among individuals initiating antiretroviral therapy in Uganda.
Methods: Sixty antiretroviral-naive HIV-infected individuals with advanced immunosuppression who were at risk of HIV-associated cognitive impairment underwent neurological, neuropsychological, and functional assessments, and gag and gp41 regions were subtyped. Subtype assignments were generated by sequence analysis using a portion of the gag and gp41 regions.
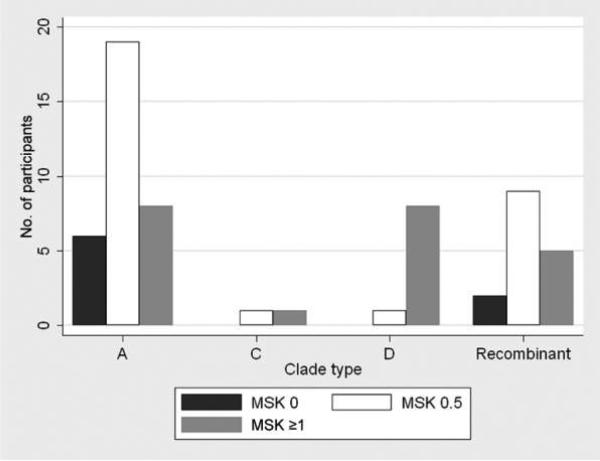
Results: Thirty-three HIV-infected individuals were infected with subtype A, 2 with subtype C, 9 with subtype D, and 16 with A/D recombinants. Eight (89%) of 9 HIV-infected individuals with subtype D had dementia, compared with 7 (24%) of 33 HIV-infected individuals with subtype A (P = .004).
Conclusions: These results suggest that, in untreated HIV-infected individuals with advanced immunosuppression who are at risk of developing HIV-associated cognitive impairment, HIV dementia may be more common among patients infected with subtype D virus than among those infected with subtype A virus. These findings provide the first evidence, to our knowledge, to demonstrate that HIV subtypes may have a pathogenetic factor with respect to their capacity to cause cognitive impairment. Additional studies are needed to confirm this observation and to define the mechanism by which subtype D leads to an increased risk of neuropathogenesis.
Figures
References
-
- Wong M, Robertson K, Nakasujja N, et al. Frequency of and risk factors for HIV dementia in an HIV clinic in sub-Saharan Africa. Neurology. 2007;68:350–5. - PubMed
-
- Liner KJ, Hall CD, Robertson KR. Impact of human immunodeficiency virus (HIV) subtypes on HIV-associated neurological disease. J Neurovirol. 2007;13:291–304. - PubMed
-
- Kiwanuka N, Laeyendecker O, Robb M, et al. Effect of Human Immunodeficiency Virus Type 1 (HIV-1) Subtype on Disease Progression in Persons from Rakai, Uganda, with Incident HIV-1 Infection. J Infect Dis. 2008;197:707–13. - PubMed
-
- Kaleebu P, French N, Mahe C, et al. Effect of human immunodeficiency virus (HIV) type 1 envelope subtypes A and D on disease progression in a large cohort of HIV-1-positive persons in Uganda. J Infect Dis. 2002;185:1244–50. - PubMed
-
- Vasan A, Renjifo B, Hertzmark E, et al. Different rates of disease progression of HIV type 1 infection in Tanzania based on infecting subtype. Clin Infect Dis. 2006;42:843–52. - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
