

Pharmacokinetics of epinephrine in patients with septic shock: modelization and interaction with endogenous neurohormonal status
- PMID: 19622169
- PMCID: PMC2750169
- DOI: 10.1186/cc7972
Pharmacokinetics of epinephrine in patients with septic shock: modelization and interaction with endogenous neurohormonal status
Abstract
Introduction: In septic patients, an unpredictable response to epinephrine may be due to pharmacodynamic factors or to non-linear pharmacokinetics. The purpose of this study was to investigate the pharmacokinetics of epinephrine and its determinants in patients with septic shock.
Methods: Thirty-eight consecutive adult patients with septic shock were prospectively recruited immediately before epinephrine infusion. A baseline blood sample (C0) was taken to assess endogenous epinephrine, norepinephrine, renin, aldosterone, and plasma cortisol levels before epinephrine infusion. At a fixed cumulative epinephrine dose adjusted to body weight and under steady-state infusion, a second blood sample (C1) was taken to assess epinephrine and norepinephrine concentrations. Data were analyzed using the nonlinear mixed effect modeling software program NONMEM.
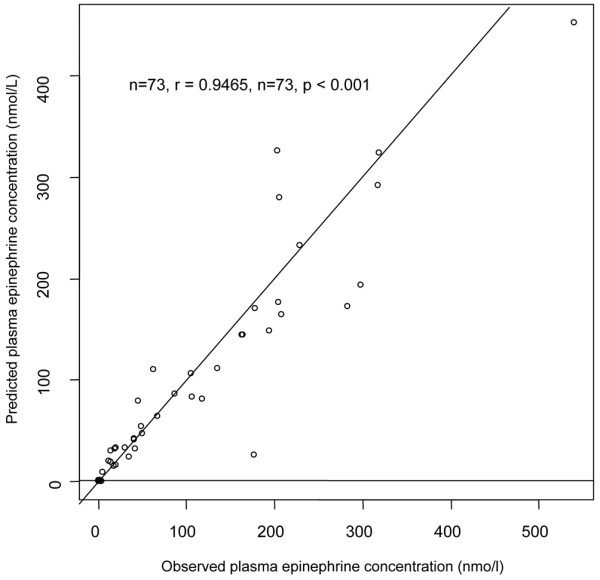
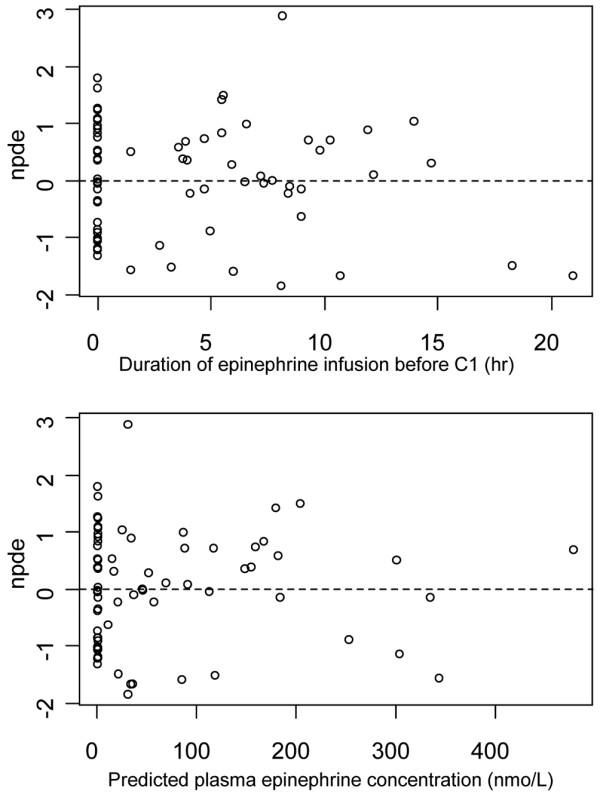
Results: Plasma epinephrine concentrations ranged from 4.4 to 540 nmol/L at steady-state infusion (range 0.1 to 7 mg/hr; 0.026 to 1.67 microg/kg/min). A one-compartment model adequately described the data. Only body weight (BW) and New Simplified Acute Physiologic Score (SAPSII) at intensive care unit admission significantly influenced epinephrine clearance: CL (L/hr) = 127 x (BW/70)0.60 x (SAPS II/50)-0.67. The corresponding half-life was 3.5 minutes. Endogenous norepinephrine plasma concentration significantly decreased during epinephrine infusion (median (range) 8.8 (1 - 56.7) at C0 vs. 4.5 (0.3 - 38.9) nmol/L at C1, P < 0.001).
Conclusions: Epinephrine pharmacokinetics is linear in septic shock patients, without any saturation at high doses. Basal neurohormonal status does not influence epinephrine pharmacokinetics. Exogenous epinephrine may alter the endogenous norepinephrine metabolism in septic patients.
Figures
Comment in
-
Epinephrine kinetics in septic shock--a means to understand variable catecholamine efficiency?Crit Care. 2009;13(4):177. doi: 10.1186/cc7987. Epub 2009 Aug 13. Crit Care. 2009. PMID: 19691814 Free PMC article.
Similar articles
-
Norepinephrine kinetics and dynamics in septic shock and trauma patients.Br J Anaesth. 2005 Dec;95(6):782-8. doi: 10.1093/bja/aei259. Epub 2005 Oct 14. Br J Anaesth. 2005. PMID: 16227334
-
Effects of dopamine, norepinephrine, and epinephrine on the splanchnic circulation in septic shock: which is best?Crit Care Med. 2003 Jun;31(6):1659-67. doi: 10.1097/01.CCM.0000063045.77339.B6. Crit Care Med. 2003. PMID: 12794401 Clinical Trial.
-
Comparison of norepinephrine and dobutamine to epinephrine for hemodynamics, lactate metabolism, and gastric tonometric variables in septic shock: a prospective, randomized study.Intensive Care Med. 1997 Mar;23(3):282-7. doi: 10.1007/s001340050329. Intensive Care Med. 1997. PMID: 9083230 Clinical Trial.
-
Dopexamine and norepinephrine versus epinephrine on gastric perfusion in patients with septic shock: a randomized study [NCT00134212].Crit Care. 2006 Feb;10(1):R32. doi: 10.1186/cc4827. Crit Care. 2006. PMID: 16507156 Free PMC article. Clinical Trial.
-
Bench-to-bedside review: Is there a place for epinephrine in septic shock?Crit Care. 2005;9(6):561-5. doi: 10.1186/cc3901. Epub 2005 Nov 4. Crit Care. 2005. PMID: 16356239 Free PMC article. Review.
Cited by
-
Epinephrine Dose Has a Preventive Effect on the Occurrence of Stress Ulcer-Induced Gastrointestinal Bleeding in Critically Ill Patients.Dig Dis Sci. 2018 Oct;63(10):2687-2694. doi: 10.1007/s10620-018-5155-8. Epub 2018 Jun 12. Dig Dis Sci. 2018. PMID: 29948567
-
Population pharmacokinetics and haemodynamic effects of norepinephrine in hypotensive critically ill children.Br J Clin Pharmacol. 2014 Oct;78(4):886-97. doi: 10.1111/bcp.12412. Br J Clin Pharmacol. 2014. PMID: 24802558 Free PMC article.
-
Evaluation of Dose Requirements Using Weight-Based versus Non-Weight-Based Dosing of Norepinephrine to Achieve a Goal Mean Arterial Pressure in Patients with Septic Shock.J Clin Med. 2023 Feb 8;12(4):1344. doi: 10.3390/jcm12041344. J Clin Med. 2023. PMID: 36835880 Free PMC article.
-
A Clinical Trial Simulation Evaluating Epinephrine Pharmacokinetics at various Dosing Frequencies during Cardiopulmonary Resuscitation.MEDtube Sci. 2016 Jun;4(2):8-15. Epub 2016 Jun 30. MEDtube Sci. 2016. PMID: 28435854 Free PMC article.
-
Epinephrine kinetics in septic shock--a means to understand variable catecholamine efficiency?Crit Care. 2009;13(4):177. doi: 10.1186/cc7987. Epub 2009 Aug 13. Crit Care. 2009. PMID: 19691814 Free PMC article.
References
-
- Annane D, Vignon P, Renault A, Bollaert PE, Charpentier C, Martin C, Troche G, Ricard JD, Nitenberg G, Papazian L, Azoulay E, Bellissant E. CATS Study Group. Norepinephrine plus dobutamine versus epinephrine alone for management of septic shock: a randomised trial. Lancet. 2007;370:676–684. doi: 10.1016/S0140-6736(07)61344-0. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
