

Selective regulation of cellular and secreted multimeric adiponectin by antidiabetic therapies in humans
- PMID: 19622782
- PMCID: PMC2739702
- DOI: 10.1152/ajpendo.00378.2009
Selective regulation of cellular and secreted multimeric adiponectin by antidiabetic therapies in humans
Abstract
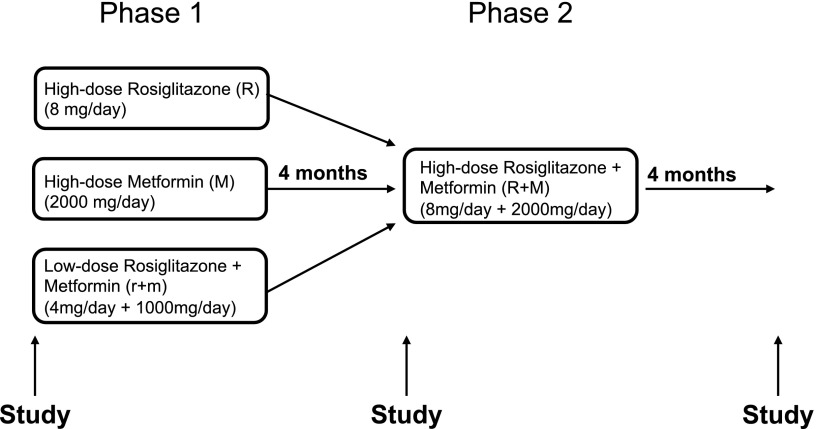
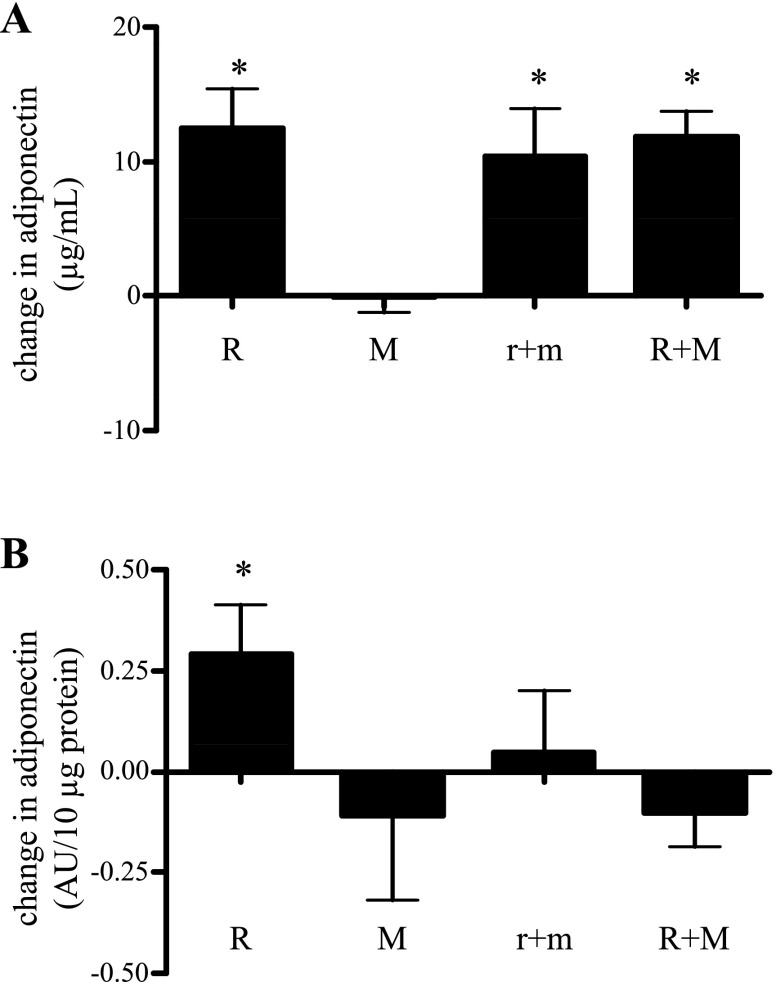
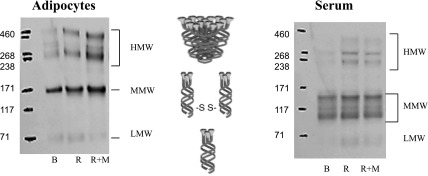
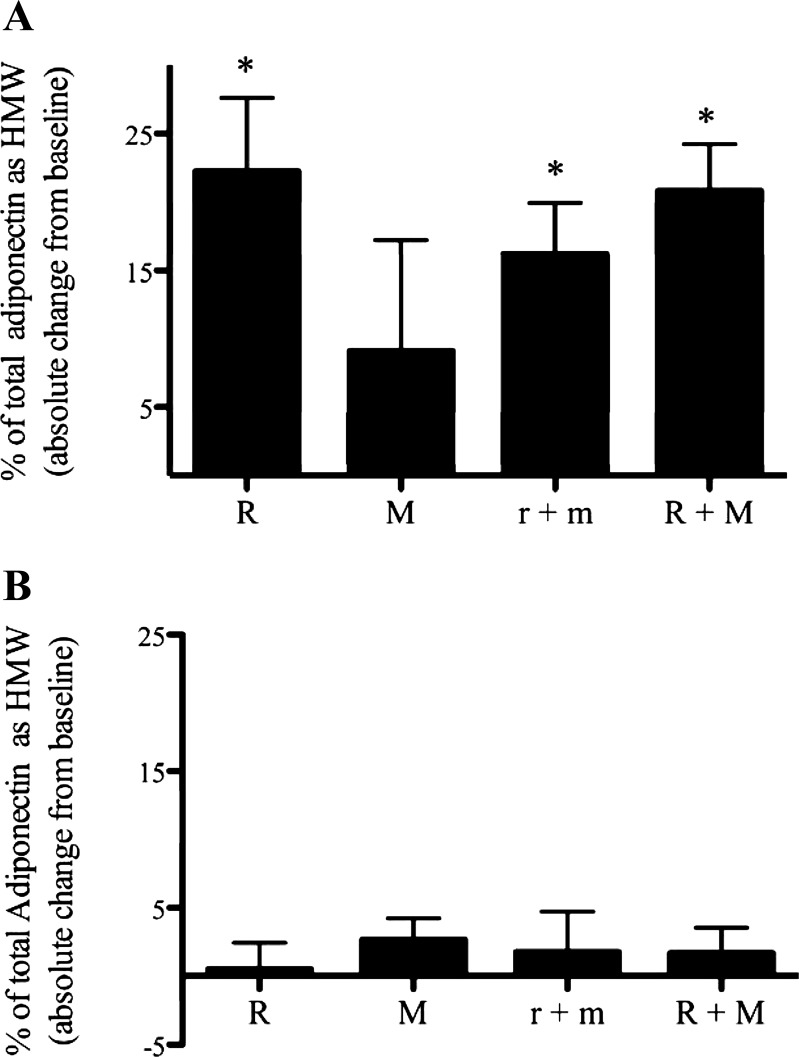
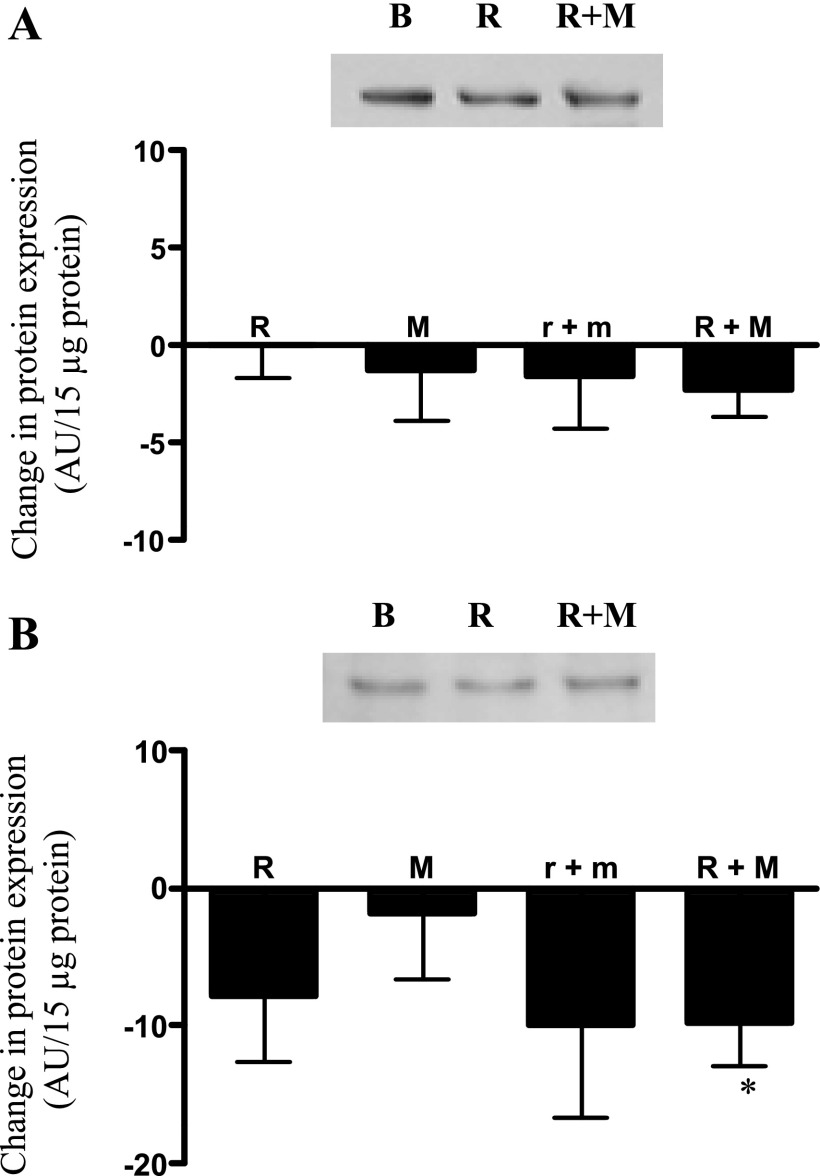
Adiponectin, an insulin-sensitizing factor secreted from adipose tissue, is decreased in individuals with type 2 diabetes (T2D) and increased in response to thiazolidinedione (TZD) therapy. Changes in its secretion and assembly into higher-order forms affect insulin sensitivity. To determine the relative potency of TZDs on intra-adipocyte multimerization and secretion of adiponectin, we assessed the impact of in vivo low- or high-dose rosiglitazone treatment alone or combined with metformin in subjects with T2D. T2D subjects received high-dose rosiglitazone (8 mg/day), high-dose metformin (2,000 mg/day), or low-dose combination rosiglitazone-metformin therapy (4 mg + 1,000 mg/day) for 4 mo. All subjects were then switched to high-dose rosiglitazone-metformin combination therapy (8 mg + 2,000 mg/day) for another 4 mo. Low-dose rosiglitazone increased serum adiponectin, whereas the high dose increased both adipocyte content and serum adiponectin levels. TZDs selectively increased the percentage of circulating adiponectin in the potent, high-molecular-weight (HMW) form. No TZD effects were evident on multimer distribution in the cell. Expression of the chaperone protein ERp44, which retains adiponectin within the cell, was decreased by TZD treatment. No changes occurred in Ero1-Lalpha expression. Metformin had no effect on any of these measures. Increases in adiponectin correlated with improvements in insulin sensitivity. In vivo, TZDs have apparent dose-dependent effects on cellular and secreted adiponectin. TZD-mediated improvements in whole body insulin sensitivity are associated with increases in circulating but not cellular levels of the HMW adiponectin multimer. Finally, TZDs promote the selective secretion of HMW adiponectin, potentially, in part, through decreasing the expression of the adiponectin-retaining protein ERp44.
Figures
References
-
- __________. Diagnosis and classification of diabetes mellitus. Diabetes Care 31, Suppl 1: S55–S60, 2008. - PubMed
-
- Abbasi F, Chang SA, Chu JW, Ciaraldi TP, Lamendola C, McLaughlin T, Reaven GM, Reaven PD. Improvements in insulin resistance with weight loss, in contrast to rosiglitazone, are not associated with changes in plasma adiponectin or adiponectin multimeric complexes. Am J Physiol Regul Integr Comp Physiol 290: R139–R144, 2006. - PubMed
-
- Bodles AM, Banga A, Rasouli N, Ono F, Kern PA, Owens RJ. Pioglitazone increases secretion of high-molecular-weight adiponectin from adipocytes. Am J Physiol Endocrinol Metab 291: E1100–E1105, 2006. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous