

Lipodystrophy: an unusual diagnosis in a case of oligomenorrhea and hirsutism
- PMID: 19622949
- PMCID: PMC2763349
- DOI: 10.1097/AOG.0b013e31819feaa9
Lipodystrophy: an unusual diagnosis in a case of oligomenorrhea and hirsutism
Abstract
Background: Familial partial lipodystrophy, Dunnigan variety, is a rare autosomal dominant disorder caused by missense mutations in LMNA gene. Individuals are predisposed to insulin resistance and its complications, including features of polycystic ovary syndrome.
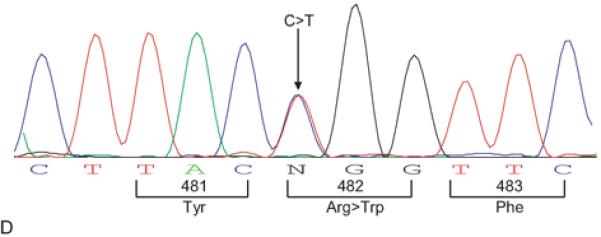
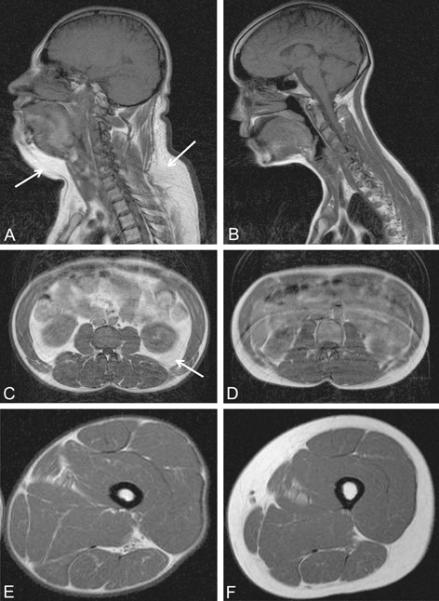
Case: A 27-year-old Hispanic woman presented with oligomenorrhea and hirsutism. Examination revealed cushingoid facies, significant hirsutism, acanthosis nigricans, and a lean body habitus. Metabolic testing identified diabetes mellitus, dyslipidemia, and steatohepatitis. A diagnosis of familial partial lipodystrophy, Dunnigan variety, was confirmed by the detection of a heterozygous p.Arg482Trp (c.1444C>T) missense mutation in the lamin A/C (LMNA) gene. Subsequently, seven female relatives were diagnosed with familial partial lipodystrophy, Dunnigan variety, four of whom had menstrual irregularities.
Conclusion: Familial partial lipodystrophy, Dunnigan variety, can present with features similar to polycystic ovary syndrome. Diagnosis is critical because the metabolic complications of the disorder have significant morbidity.
Figures


Similar articles
-
Polycystic ovary syndrome in familial partial lipodystrophy type 2 (FPLD2): basic and clinical aspects.Nucleus. 2018;9(1):392-397. doi: 10.1080/19491034.2018.1509659. Nucleus. 2018. PMID: 30131000 Free PMC article. Review.
-
Familial partial lipodystrophy as differential diagnosis of polycystic ovary syndrome.Endokrynol Pol. 2015;66(6):550-4. doi: 10.5603/EP.2015.0067. Endokrynol Pol. 2015. PMID: 26662654
-
[Familial partial lipodystrophy (Dunnigan syndrome) due to LMNA gene mutation: The first description of its clinical case in Russia].Ter Arkh. 2015;87(3):83-87. doi: 10.17116/terarkh201587383-87. Ter Arkh. 2015. PMID: 26027246 Russian.
-
Dunnigan-type familial partial lipodystrophy associated with the heterozygous R482W mutation in LMNA gene - case study of three women from one family.Endokrynol Pol. 2013;64(4):306-11. doi: 10.5603/ep.2013.0010. Endokrynol Pol. 2013. PMID: 24002959
-
Hypopharyngeal Squamous Cell Carcinoma in Sisters with LMNA Associated Familial Partial Lipodystrophy: A Case Report and Review of the Literature.Ann Otol Rhinol Laryngol. 2020 Dec;129(12):1243-1246. doi: 10.1177/0003489420933645. Epub 2020 Jun 9. Ann Otol Rhinol Laryngol. 2020. PMID: 32517491 Review.
Cited by
-
Polycystic ovary syndrome in familial partial lipodystrophy type 2 (FPLD2): basic and clinical aspects.Nucleus. 2018;9(1):392-397. doi: 10.1080/19491034.2018.1509659. Nucleus. 2018. PMID: 30131000 Free PMC article. Review.
-
Deciphering the Clinical Presentations in LMNA-related Lipodystrophy: Report of 115 Cases and a Systematic Review.J Clin Endocrinol Metab. 2024 Feb 20;109(3):e1204-e1224. doi: 10.1210/clinem/dgad606. J Clin Endocrinol Metab. 2024. PMID: 37843397 Free PMC article.
-
Lipodystrophies, dyslipidaemias and atherosclerotic cardiovascular disease.Pathology. 2019 Feb;51(2):202-212. doi: 10.1016/j.pathol.2018.11.004. Epub 2018 Dec 27. Pathology. 2019. PMID: 30595509 Free PMC article. Review.
References
-
- Dunnigan MG, Cochrane M, Kelly A, Scott JW. Familial lipoatrophic diabetes with dominant transmission. Q J Med. 1974;49:33–48. - PubMed
-
- Garg A. Acquired and Inherited Lipodystrophies. New England Journal of Medicine. 2004;350:1220–43. - PubMed
-
- Garg A. Gender Differences in the Prevalence of Metabolic Complications in Familial Partial Lipodystrophy (Dunnigan Variety) J of Clin Endoc & Metab. 2000;86:1776–81. - PubMed
-
- Pasquali R. Obesity and Androgens: Facts and Perspectives. Fertil Steril. 2006;85:1319–36. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
