

Longitudinal shapes of the tibia and femur are unrelated and variable
- PMID: 19623495
- PMCID: PMC2835607
- DOI: 10.1007/s11999-009-0984-6
Longitudinal shapes of the tibia and femur are unrelated and variable
Abstract
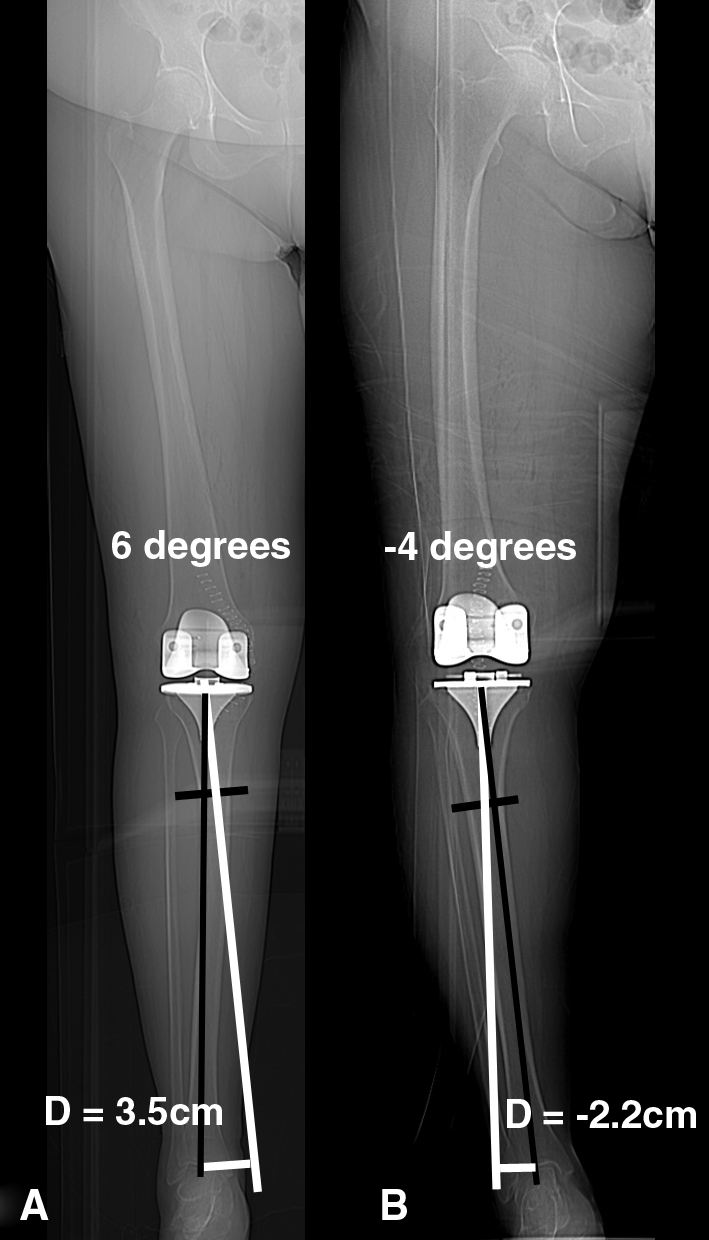
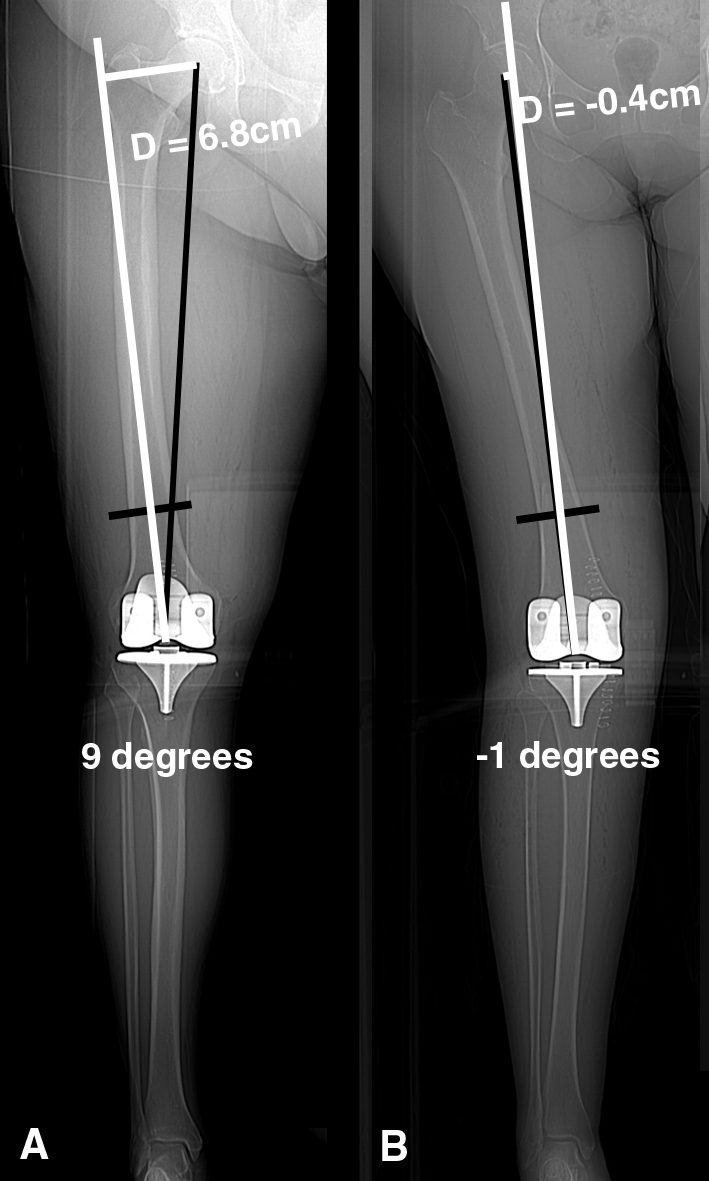
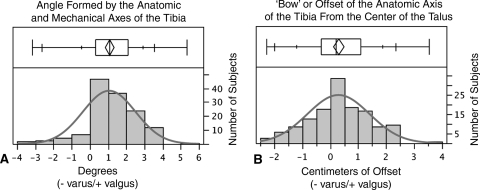
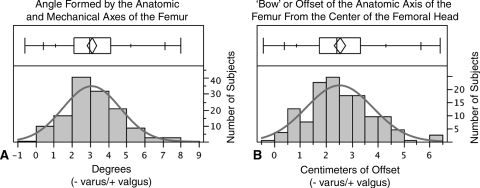
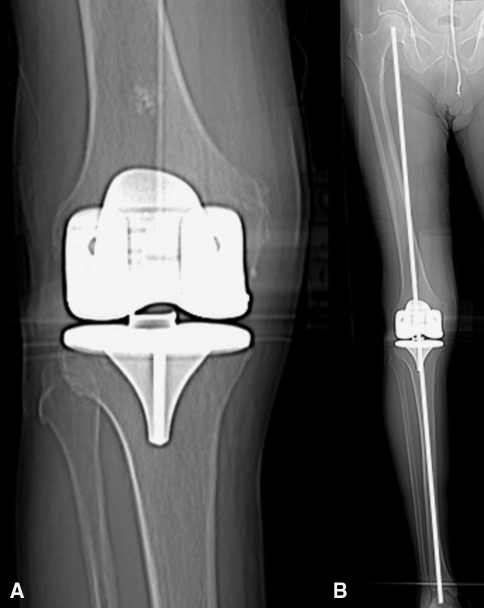
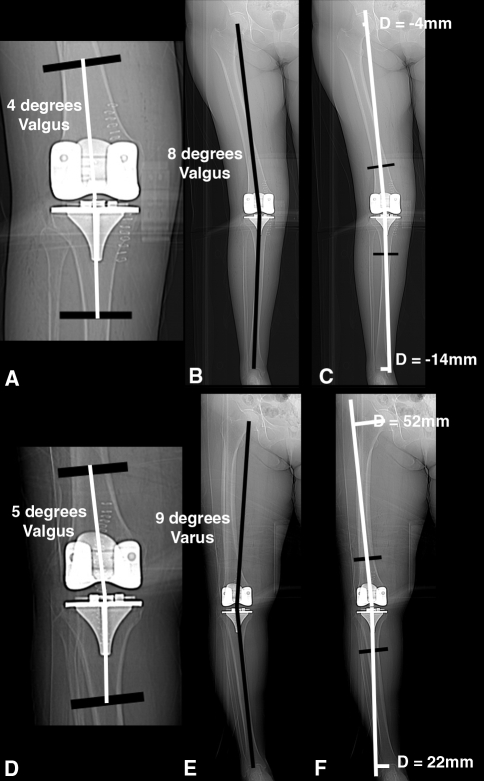
In general practice, short films of the knee are used to assess component position and define the entry point for intramedullary femoral alignment in TKAs; however, whether it is justified to use the short film commonly used in research settings and everyday practice as a substitute for the whole leg view is controversial and needs clarification. In 138 long leg CT scanograms we measured the angle formed by the anatomic axis of the proximal fourth of the tibia and the mechanical axis of the tibia, the angle formed by the anatomic axis of the distal fourth of the femur and the mechanical axis of the femur, the "bow" of the tibia (as reflected by the offset of the anatomic axis from the center of the talus), and the "bow" of the femur (as reflected by the offset of the anatomic axis from the center of the femoral head). Because the angle formed by these axes and the bow of the tibia and femur have wide variability in females and males, a short film of the knee should not be used in place of the whole leg view when accurate assessment of component position and limb alignment is essential. A previous study of normal limbs found that only 2% of subjects have a neutral hip-knee-ankle axis, which can be explained by the wide variability of the bow in the tibia and femur and the lack of correlation between the bow of the tibia and femur in a given limb as shown in the current study.
Figures
Similar articles
-
Trabecular orientation in the human femur and tibia and the relationship with lower-limb alignment for patients with osteoarthritis of the knee.J Biomech. 2015 Apr 13;48(6):1214-8. doi: 10.1016/j.jbiomech.2015.01.028. Epub 2015 Feb 2. J Biomech. 2015. PMID: 25721769
-
Mismatch between femur and tibia coronal alignment in the knee joint: classification of five lower limb types according to femoral and tibial mechanical alignment.BMC Musculoskelet Disord. 2018 Nov 24;19(1):411. doi: 10.1186/s12891-018-2335-9. BMC Musculoskelet Disord. 2018. PMID: 30474544 Free PMC article.
-
Neutral alignment resulting from tibial vara and opposite femoral valgus is the main morphologic pattern in healthy middle-aged patients: an exploration of a 3D-CT database.Knee Surg Sports Traumatol Arthrosc. 2021 Mar;29(3):849-858. doi: 10.1007/s00167-020-06030-4. Epub 2020 May 5. Knee Surg Sports Traumatol Arthrosc. 2021. PMID: 32372282
-
Highly variable coronal tibial and femoral alignment in osteoarthritic knees: a systematic review.Knee Surg Sports Traumatol Arthrosc. 2019 May;27(5):1368-1377. doi: 10.1007/s00167-019-05506-2. Epub 2019 Apr 15. Knee Surg Sports Traumatol Arthrosc. 2019. PMID: 30989273
-
High variability exists in 3D leg alignment analysis, but underlying principles that might lead to agreement on a universal framework could be identified: A systematic review.Knee Surg Sports Traumatol Arthrosc. 2025 Jun;33(6):2063-2077. doi: 10.1002/ksa.12512. Epub 2024 Oct 26. Knee Surg Sports Traumatol Arthrosc. 2025. PMID: 39460613 Free PMC article.
Cited by
-
Physiological joint line total knee arthroplasty designs are especially sensitive to rotational placement - A finite element analysis.PLoS One. 2018 Feb 5;13(2):e0192225. doi: 10.1371/journal.pone.0192225. eCollection 2018. PLoS One. 2018. PMID: 29401510 Free PMC article.
-
Lateral Coronal Bowing of Femur and/or Tibia Amplifies the Varus Malalignment of Lower Limb as well as Increases Functional Disability in Patients with Knee Osteoarthritis.Indian J Orthop. 2020 Nov 22;55(Suppl 1):88-96. doi: 10.1007/s43465-020-00303-3. eCollection 2021 May. Indian J Orthop. 2020. PMID: 34122760 Free PMC article.
-
Femoral shaft bowing in the coronal plane has more significant effect on the coronal alignment of TKA than proximal or distal variations of femoral shape.Knee Surg Sports Traumatol Arthrosc. 2015 Jul;23(7):1936-42. doi: 10.1007/s00167-014-3006-5. Epub 2014 Apr 24. Knee Surg Sports Traumatol Arthrosc. 2015. PMID: 24760162
-
Assessment of lower limb alignment: supine weight-bearing CT scanograms compared with a standing full-length radiograph.Skeletal Radiol. 2024 Aug;53(8):1465-1471. doi: 10.1007/s00256-024-04637-z. Epub 2024 Mar 5. Skeletal Radiol. 2024. PMID: 38443696 Review.
-
Coronal Alignment of the Lower Extremity: A Gender-Based Radio-Graphic Analysis in Indian Patients.Indian J Orthop. 2020 Mar 10;54(4):504-512. doi: 10.1007/s43465-020-00050-5. eCollection 2020 Jul. Indian J Orthop. 2020. PMID: 32549966 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
