

Using CT colonography as a triage technique after a positive faecal occult blood test in colorectal cancer screening
- PMID: 19625276
- PMCID: PMC2719082
- DOI: 10.1136/gut.2009.176867
Using CT colonography as a triage technique after a positive faecal occult blood test in colorectal cancer screening
Abstract
Objective: The purpose of this study was to evaluate the effectiveness of CT colonography (CTC) as a triage technique in faecal occult blood test (FOBT)-positive screening participants.
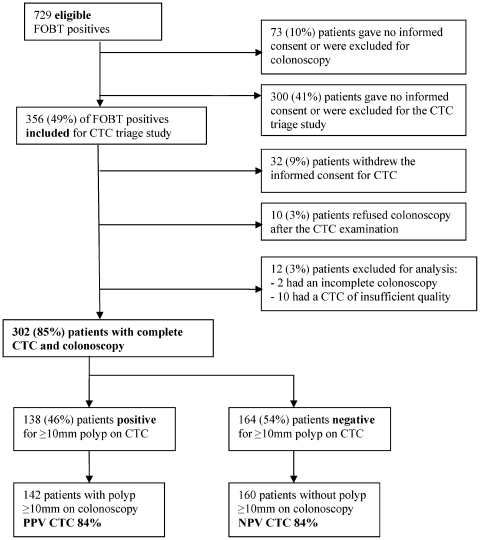
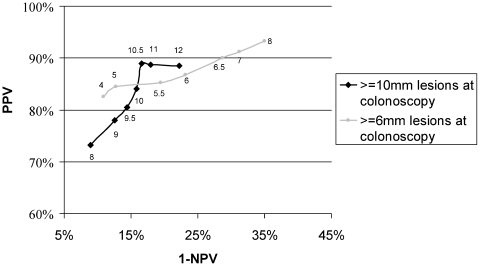
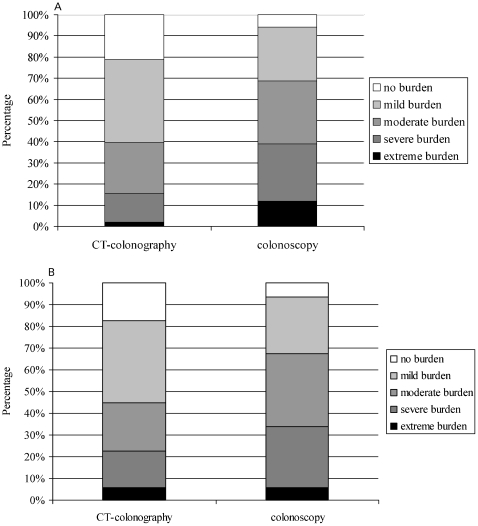
Methods: Consecutive guaiac (G-FOBT) and immunochemical (I-FOBT) FOBT-positive patients scheduled for colonoscopy underwent CTC with iodine tagging bowel preparation. Each CTC was read independently by two experienced observers. Per patient sensitivity, specificity and positive and negative predictive values (PPV and NPV) were calculated based on double reading with different CTC cut-off lesion sizes using segmental unblinded colonoscopy as the reference standard. The acceptability of the technique to patients was evaluated with questionnaires.
Results: 302 FOBT-positive patients were included (54 G-FOBT and 248 I-FOBT). 22 FOBT-positive patients (7%) had a colorectal carcinoma and 211 (70%) had a lesion >or=6 mm. Participants considered colonoscopy more burdensome than CTC (p<0.05). Using a 6 mm CTC size cut-off, per patient sensitivity for CTC was 91% (95% CI 85% to 91%) and specificity was 69% (95% CI 60% to 89%) for the detection of colonoscopy lesions >or=6 mm. The PPV of CTC was 87% (95% CI 80% to 93%) and NPV 77% (95% CI 69% to 85%). Using CTC as a triage technique in 100 FOBT-positive patients would mean that colonoscopy could be prevented in 28 patients while missing >or=10 mm lesions in 2 patients.
Conclusion: CTC with limited bowel preparation has reasonable predictive values in an FOBT-positive population and a higher acceptability to patients than colonoscopy. However, due to the high prevalence of clinically relevant lesions in FOBT-positive patients, CTC is unlikely to be an efficient triage technique in a first round FOBT population screening programme.
Conflict of interest statement
Figures
References
-
- Winawer S, Fletcher R, Rex D, et al. Colorectal cancer screening and surveillance: clinical guidelines and rationale. Update based on new evidence. Gastroenterology 2003;124:544–60 - PubMed
-
- Bond JH. Polyp guideline: diagnosis, treatment, and surveillance for patients with colorectal polyps. Practice Parameters Committee of the American College of Gastroenterology. Am J Gastroenterol 2000;95:3053–63 - PubMed
-
- Hardcastle JD, Chamberlain JO, Robinson MH, et al. Randomised controlled trial of faecal-occult-blood screening for colorectal cancer. Lancet 1996;348:1472–7 - PubMed
-
- Heresbach D, Manfredi S, D’halluin PN, et al. Review in depth and meta-analysis of controlled trials on colorectal cancer screening by faecal occult blood test. Eur J Gastroenterol Hepatol 2006;18:427–33 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical