

Determining the rise in BCR-ABL RNA that optimally predicts a kinase domain mutation in patients with chronic myeloid leukemia on imatinib
- PMID: 19625707
- PMCID: PMC2756120
- DOI: 10.1182/blood-2008-08-173674
Determining the rise in BCR-ABL RNA that optimally predicts a kinase domain mutation in patients with chronic myeloid leukemia on imatinib
Abstract
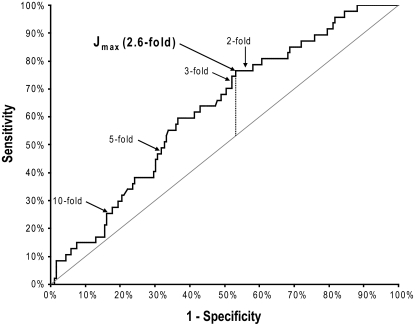
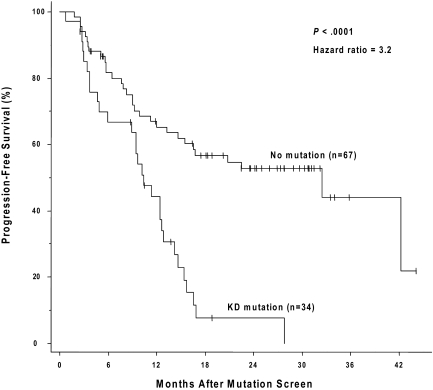
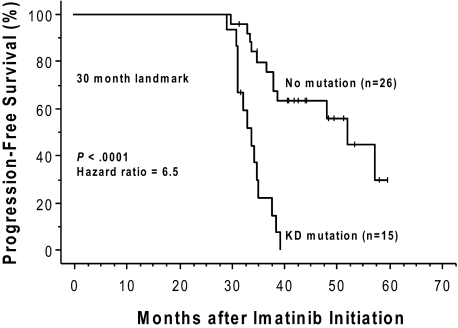
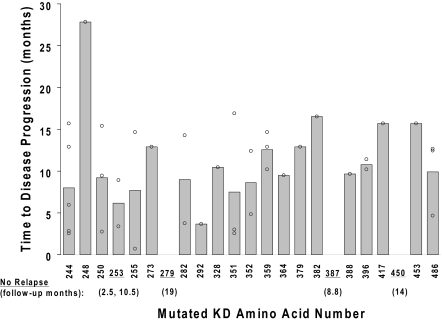
In imatinib-treated chronic myeloid leukemia (CML), secondary drug resistance is often caused by mutations in the BCR-ABL kinase domain (KD). As alternative therapies are available for imatinib resistance, early identification of mutations may prevent disease progression. Because most patients are routinely monitored by BCR-ABL quantitative polymerase chain reaction (PCR), it is important to define the optimal increase in BCR-ABL that should trigger mutation testing. Expert panels have provisionally recommended a 10-fold BCR-ABL increase as the trigger for mutation screening, acknowledging the lack of consensus. To address this question, we monitored 150 CML patients by quantitative PCR and DNA sequencing. Thirty-five different mutations were identified in 53 patients, and, during 22.5 months (median) of follow-up after sequencing, mutations were significantly predictive of shorter progression-free survival. An unbiased receiver operating characteristic analysis identified a 2.6-fold increase in BCR-ABL RNA as the optimal cutoff for predicting a concomitant KD mutation, with a sensitivity of 77% (94% if including subsequent samples). The 2.6-fold threshold approximated the analytic precision limit of our PCR assay. In contrast, transcript rise cutoffs of 5-fold or greater had poor diagnostic sensitivity and no significant association with mutations. We conclude that the currently recommended 10-fold threshold to trigger mutation screening is insensitive and not universally applicable.
Figures
References
-
- Apperley JF. Part I: mechanisms of resistance to imatinib in chronic myeloid leukaemia. Lancet Oncol. 2007;8(11):1018–1029. - PubMed
-
- O'Hare T, Eide CA, Deininger MW. Bcr-Abl kinase domain mutations, drug resistance and the road to a cure of chronic myeloid leukemia. Blood. 2007;110(7):2242–2249. - PubMed
-
- Baccarani M, Saglio G, Goldman J, et al. Evolving concepts in the management of chronic myeloid leukemia: recommendations from an expert panel on behalf of the European LeukemiaNet. Blood. 2006;108(6):1809–1820. - PubMed
-
- Hughes TP, Deininger MW, Hochhaus A, et al. Monitoring CML patients responding to treatment with tyrosine kinase inhibitors: review and recommendations for ‘harmonizing’ current methodology for detecting BCR-ABL transcripts and kinase domain mutations and for expressing results. Blood. 2006;108(1):28–37. - PMC - PubMed
-
- O'Brien S. NCCN Clinical Practice Guidelines in Oncology: Chronic Myelogenous Leukemia. Version 2.2010. [Accessed July 2009]. http://www.nccn.org/professionals/physician_gls/PDF/cml.pdf. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
