

Degenerative lumbar spinal stenosis: current strategies in diagnosis and treatment
- PMID: 19626175
- PMCID: PMC2696879
- DOI: 10.3238/arztebl.2008.0373
Degenerative lumbar spinal stenosis: current strategies in diagnosis and treatment
Abstract
Introduction: Although the aging of the population is causing a dramatic rise in the incidence of lumbar spinal stenosis, the indications and options for surgical treatment are not clearly defined.
Methods: In an attempt to aid clinical decision making, a selective literature review was conducted, taking into account the guidelines of the Association of the Scientific Medical Societies in Germany (AWMF).
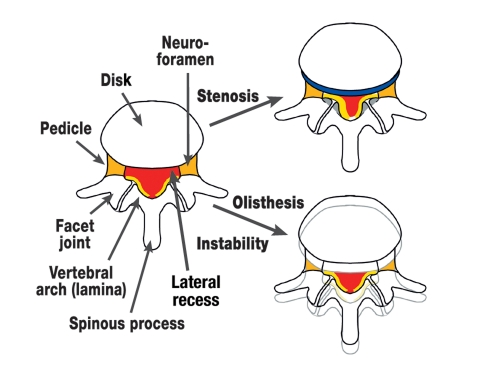
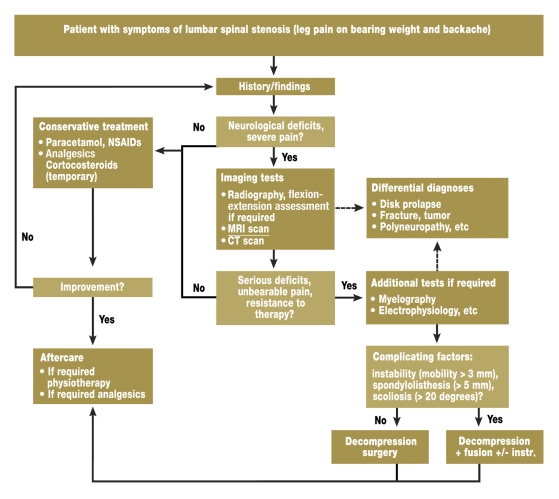
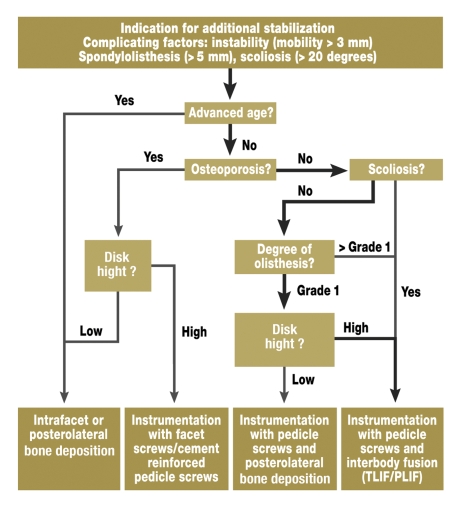
Results: In degenerative lumbar spinal stenosis hypertrophy of the facet joints and yellow ligaments brings about constriction of the spinal canal, leading to back pain and activity-dependent lower limb symptoms (neurogenic claudication). If conservative treatment fails, an imaging study, usually magnetic resonance imaging, is required. In the case of severe symptoms the progressive underlying degeneration necessitates surgical treatment. Minimally invasive fenestration techniques are usually employed to decompress the spinal canal; in the presence of instability, fusion is indicated.
Discussion: Despite the proven superiority of surgery in the management of refractory lumbar spinal stenosis, there is a lack of evidence-based data regarding the different surgical treatment options. The evaluation of modern, minimally invasive techniques is thus difficult.
Keywords: fenestration; fusion; laminectomy; lumbar spinal stenosis; neurogenic claudication; surgery.
Figures
References
-
- Boden SD, Davis DO, Dina TS, Patronas NJ, Wiesel SW. Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects. A prospective investigation. J Bone Joint Surg Am. 1990;72:403–408. - PubMed
-
- Ciol MA, Deyo RA, Howell E, Kreif S. An assessment of surgery for spinal stenosis: time trends, geographic variations, complications, and reoperations. J Am Geriatr Soc. 1996;44:285–290. - PubMed
-
- AWMF-Leitlinie. Leitlinien der Deutschen Gesellschaft für Neurochirurgie „Lumbale Spinalkanalstenose“ http://www.uni-duesseldorf.de/awmf/ll-na/008-022.htm. 2005.
-
- Porter RW. Spinal stenosis and neurogenic claudication. Spine. 1996;21:2046–2052. - PubMed
-
- Benoist M. The natural history of lumbar degenerative spinal stenosis. Joint Bone Spine. 2002;69:450–457. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources