

Depth of tumor invasion better predicts prognosis than the current American Joint Committee on Cancer T classification for distal bile duct carcinoma
- PMID: 19628081
- PMCID: PMC3402913
- DOI: 10.1016/j.surg.2009.02.023
Depth of tumor invasion better predicts prognosis than the current American Joint Committee on Cancer T classification for distal bile duct carcinoma
Abstract
Background: The American Joint Committee on Cancer (AJCC) T classification system for cholangiocarcinoma does not take into account the unique pathologic features of the bile duct. As such, the current AJCC T classification for distal cholangiocarcinoma may be inaccurate.
Methods: A total of 147 patients with distal cholangiocarcinoma were identified from a single institution database. The prognostic importance of depth of tumor invasion relative to the AJCC T classification system was assessed.
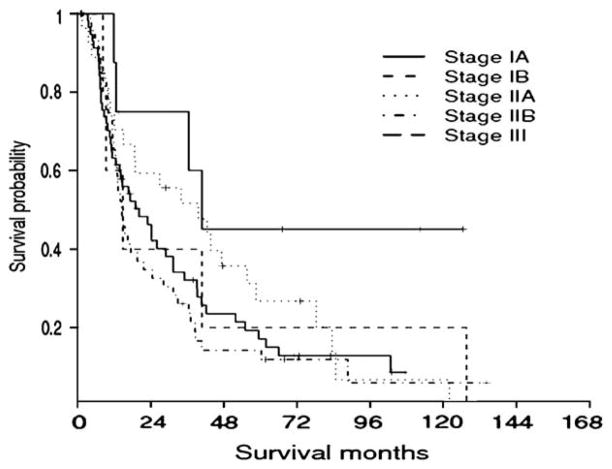
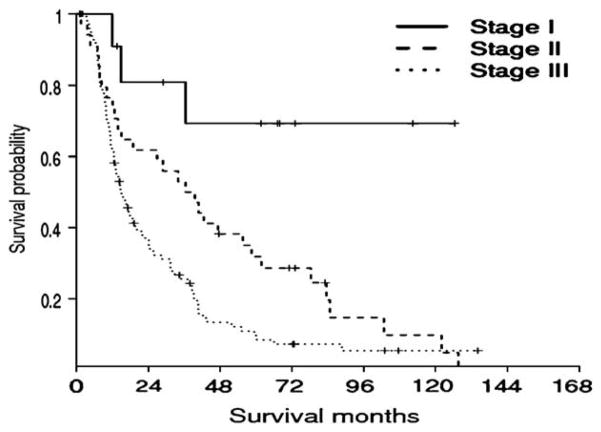
Results: The AJCC T classification was T1 (n = 11, 7.5%), T2 (n = 6, 4.1%), T3 (n = 73, 49.7%), or T4 (n = 57, 38.8%). When cases were analyzed according to depth of tumor invasion, most lesions were > or =5 mm (<5 mm, 9.5%; range, 5-12, 51.0%; >12 mm, 39.5%). The AJCC T classification was not associated with survival outcome (median survival, T1, 40.1 months; T2, 14.8 months; T3, 16.5 months; T4, 20.2 months; P = .17). In contrast, depth of tumor invasion was associated with a worse outcome as tumor depth increased (median survival, <5 mm, not reached; range, 5-12, 28.9 months; >12 mm, 12.9 months; P = .001). On multivariate analyses, tumor depth remained the factor most associated with outcome (<5 mm; hazard ratio [HR] = referent vs 5-12 mm; HR = 3.8 vs >12 mm; HR = 6.7 mm; P = .001).
Conclusion: The AJCC T classification for distal cholangiocarcinoma does not accurately predict prognosis. Depth of the bile duct carcinoma invasion is a better alternative method to determine prognosis and should be incorporated into the pathologic assessment of resected distal cholangiocarcinoma.
Figures


Similar articles
-
Pancreatic and duodenal invasion in distal bile duct cancer: paradox in the tumor classification of the American Joint Committee on Cancer.World J Surg. 2007 Oct;31(10):2008-15. doi: 10.1007/s00268-007-9173-5. World J Surg. 2007. PMID: 17661132
-
Proposal for a new T-stage classification system for distal cholangiocarcinoma: a 10-institution study from the U.S. Extrahepatic Biliary Malignancy Consortium.HPB (Oxford). 2016 Oct;18(10):793-799. doi: 10.1016/j.hpb.2016.07.009. Epub 2016 Aug 9. HPB (Oxford). 2016. PMID: 27506989 Free PMC article.
-
Validation of the T category for distal cholangiocarcinoma: Measuring the depth of invasion is complex but correlates with survival.Ann Diagn Pathol. 2020 Jun;46:151489. doi: 10.1016/j.anndiagpath.2020.151489. Epub 2020 Mar 3. Ann Diagn Pathol. 2020. PMID: 32169826
-
[TNM staging of hilar cholangiocarcinoma].Korean J Gastroenterol. 2005 Jul;46(1):20-7. Korean J Gastroenterol. 2005. PMID: 16030400 Review. Korean.
-
Intrahepatic cholangiocarcinoma: macroscopic type and stage classification.J Hepatobiliary Pancreat Surg. 2003;10(4):288-91. doi: 10.1007/s00534-002-0732-8. J Hepatobiliary Pancreat Surg. 2003. PMID: 14598147 Review.
Cited by
-
Diagnostic and prognostic value of MCM3 and its interacting proteins in hepatocellular carcinoma.Oncol Lett. 2020 Dec;20(6):308. doi: 10.3892/ol.2020.12171. Epub 2020 Sep 30. Oncol Lett. 2020. PMID: 33093917 Free PMC article.
-
Hilar cholangiocarcinoma: tumor depth as a predictor of outcome.Arch Surg. 2011 Jun;146(6):697-703. doi: 10.1001/archsurg.2011.122. Arch Surg. 2011. PMID: 21690446 Free PMC article.
-
Indications for resection of recurrent lesions in patients with distal cholangiocarcinoma based on prognostic factors: a single-institute retrospective study and brief literature review.BMC Surg. 2022 Dec 12;22(1):423. doi: 10.1186/s12893-022-01879-3. BMC Surg. 2022. PMID: 36503431 Free PMC article.
-
Cholangiocarcinoma: a site-specific update on the current state of surgical management and multi-modality therapy.Chin Clin Oncol. 2020 Feb;9(1):4. doi: 10.21037/cco.2019.08.09. Epub 2019 Sep 2. Chin Clin Oncol. 2020. PMID: 31500433 Free PMC article. Review.
-
Resection for Klatskin tumors: technical complexities and results.Transl Gastroenterol Hepatol. 2018 Sep 18;3:69. doi: 10.21037/tgh.2018.09.01. eCollection 2018. Transl Gastroenterol Hepatol. 2018. PMID: 30363698 Free PMC article. Review.
References
-
- Farley DR, Weaver AL, Nagorney DM. “Natural history” of unresected cholangiocarcinoma: patient outcome after noncurative intervention. Mayo Clin Proc. 1995;70:425–9. - PubMed
-
- Patel T. Increasing incidence and mortality of primary intra-hepatic cholangiocarcinoma in the United States. Hepatology. 2001;33:1353–7. - PubMed
-
- Sugiura Y, Nakamura S, Iida S, et al. Extensive resection of the bile ducts combined with liver resection for cancer of the main hepatic duct junction: a cooperative study of the Keio Bile Duct Cancer Study Group. Surgery. 1994;115:445–51. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
