

Clinical and genetic modifiers of long-term survival in heart failure
- PMID: 19628119
- PMCID: PMC2749467
- DOI: 10.1016/j.jacc.2009.05.009
Clinical and genetic modifiers of long-term survival in heart failure
Abstract
Objectives: This study sought to identify genetic modifiers of beta-blocker response and long-term survival in heart failure (HF).
Background: Differences in beta-blocker treatment effect between Caucasians and African Americans with HF have been reported.
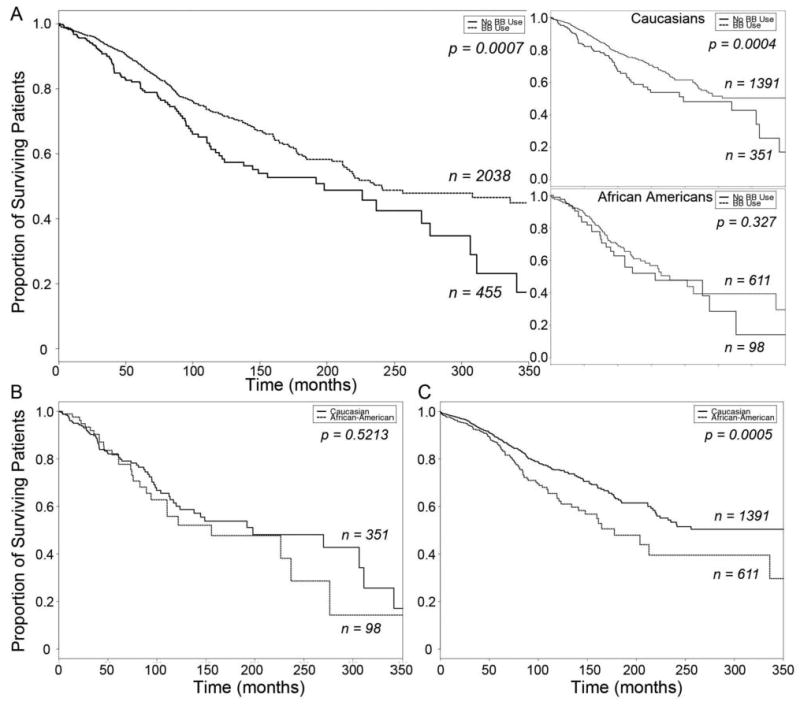
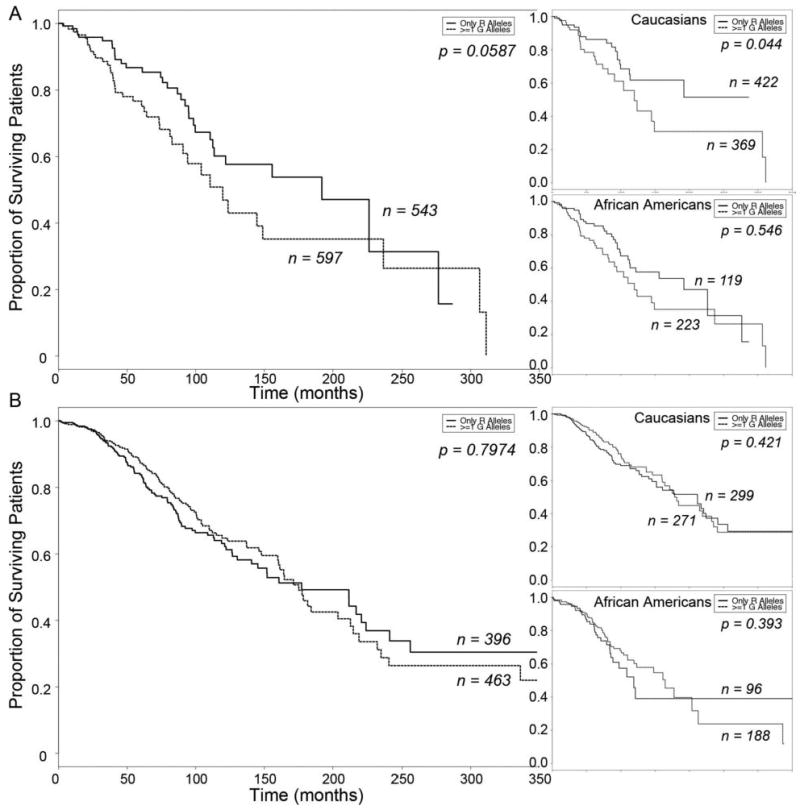
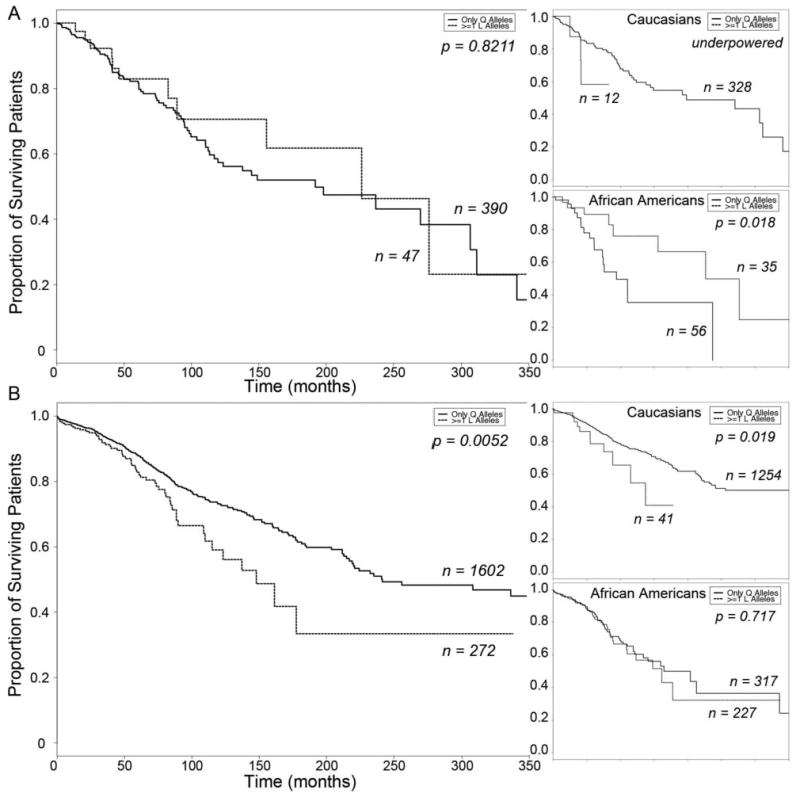
Methods: This was a prospective cohort study of 2,460 patients (711 African American, 1,749 Caucasian) enrolled between 1999 and 2007; 2,039 patients (81.7%) were treated with a beta-blocker. Each was genotyped for beta1-adrenergic receptor (ADRB1) Arg389>Gly and G-protein receptor kinase 5 (GRK5) Gln41>Leu polymorphisms, which are more prevalent among African Americans than Caucasians. The primary end point was survival time from HF onset.
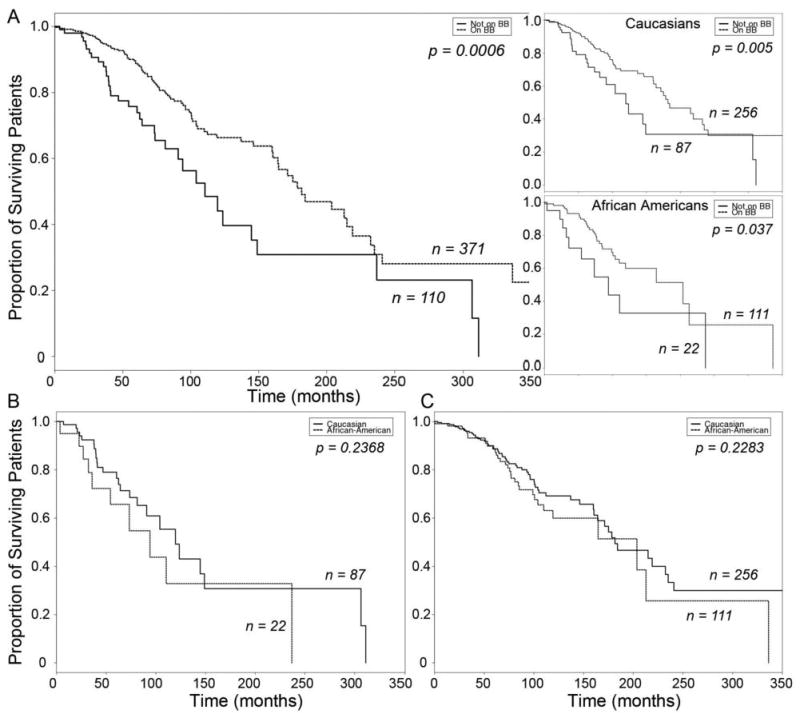
Results: There were 765 deaths during follow-up (median 46 months). beta-blocker treatment increased survival in Caucasians (log-rank p = 0.00038) but not African Americans (log-rank p = 0.327). Among patients not taking beta-blockers, ADRB1 Gly389 was associated with decreased survival in Caucasians (hazard ratio [HR]: 1.98, 95% confidence interval [CI]: 1.1 to 3.7, p = 0.03) whereas GRK5 Leu41 was associated with improved survival in African Americans (HR: 0.325, CI: 0.133 to 0.796, p = 0.01). African Americans with ADRB1 Gly389Gly GRK5 Gln41Gln derived a similar survival benefit from beta-blocker therapy (HR: 0.385, 95% CI: 0.182 to 0.813, p = 0.012) as Caucasians with the same genotype (HR: 0.529, 95% CI: 0.326 to 0.858, p = 0.0098).
Conclusions: These data show that differences caused by beta-adrenergic receptor signaling pathway gene polymorphisms, rather than race, are the major factors contributing to apparent differences in the beta-blocker treatment effect between Caucasians and African Americans; proper evaluation of treatment response should account for genetic variance.
Figures
References
-
- American Heart Association. Dallas, Texas: American Heart Association; 2001. 2002 Heart and Stroke Statistical Update. Available at: http://heartnet.bjmu.edu.cn/epi/usa/2002update.htm.
-
- Kaye DM, Smirk B, Finch S, Williams C, Esler MD. Interaction between cardiac sympathetic drive and heart rate in heart failure: modulation by adrenergic receptor genotype. J Am Coll Cardiol. 2004;44:2008–15. - PubMed
-
- Lefkowitz RJ, Rockman HA, Koch WJ. Catecholamines, cardiac beta-adrenergic receptors, and heart failure. Circulation. 2000;101:1634–7. - PubMed
-
- Bristow MR. beta-adrenergic receptor blockade in chronic heart failure. Circulation. 2000;101:558–69. - PubMed
-
- Domanski MJ, Krause-Steinrauf H, Massie BM, et al. A comparative analysis of the results from 4 trials of beta-blocker therapy for heart failure: BEST, CIBIS-II, MERIT-HF, and COPERNICUS. J Card Fail. 2003;9:354–63. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
