

Prevalence and pathophysiologic attributes of ventricular dyssynchrony in arrhythmogenic right ventricular dysplasia/cardiomyopathy
- PMID: 19628120
- PMCID: PMC4138506
- DOI: 10.1016/j.jacc.2009.04.038
Prevalence and pathophysiologic attributes of ventricular dyssynchrony in arrhythmogenic right ventricular dysplasia/cardiomyopathy
Abstract
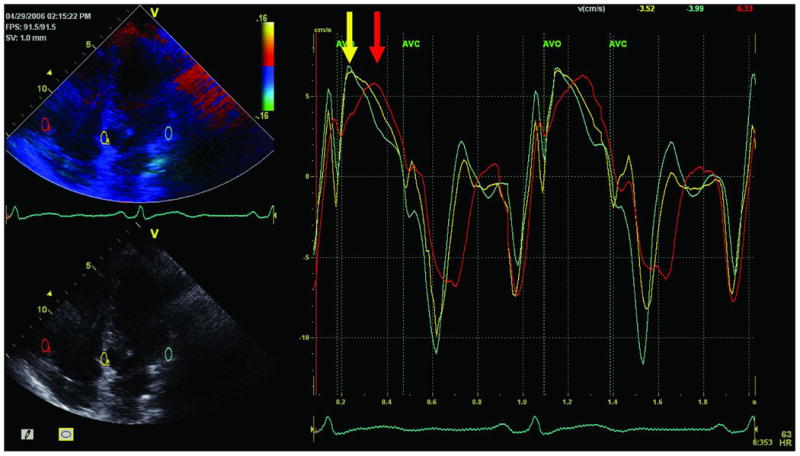
Objectives: This study sought to investigate the prevalence and mechanisms underlying right ventricular (RV) dyssynchrony in arrhythmogenic right ventricular dysplasia/cardiomyopathy (ARVD/C) using tissue Doppler echocardiography (TDE).
Background: An ARVD/C is characterized by fibrofatty replacement of RV myocardium and RV dilation. These pathologic changes may result in electromechanical dyssynchrony.
Methods: Echocardiography, both conventional and TDE, was performed in 52 ARVD/C patients fulfilling Task Force criteria and 25 control subjects. The RV end-diastolic and -systolic areas, right ventricular fractional area change (RVFAC), and left ventricular (LV) volumes and function were assessed. Mechanical synchrony was assessed by measuring differences in time-to-peak systolic velocity (T(SV)) between the RV free wall, ventricular septum, and LV lateral wall. An RV dyssynchrony was defined as the difference in T(SV) between the RV free wall and the ventricular septum, >2 SD above the mean value for control subjects.
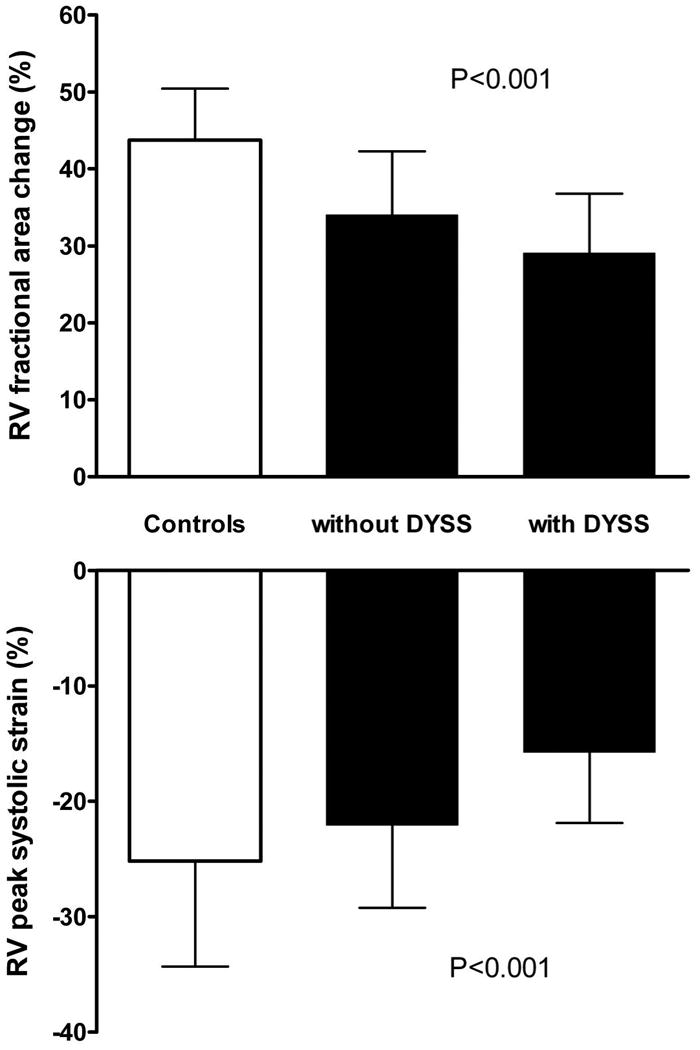
Results: The mean difference in RV T(SV) was higher in ARVD/C compared with control subjects (55 +/- 34 ms vs. 26 +/- 15 ms, p < 0.001). Significant RV dyssynchrony was not noted in any of the control subjects. Based on a cutoff value of 56 ms, significant RV dyssynchrony was present in 26 ARVD/C patients (50%). Patients with RV dyssynchrony had a larger RV end-diastolic area (22 +/- 5 cm(2) vs. 19 +/- 4 cm(2), p = 0.02), and lower RVFAC (29 +/- 8% vs. 34 +/- 8%, p = 0.03) compared with ARVD/C patients without RV dyssynchrony. No differences in QRS duration, LV volumes, or function were present between the 2 groups.
Conclusions: An RV dyssynchrony may occur in up to 50% of ARVD/C patients, and is associated with RV remodeling. This finding may have therapeutic and prognostic implications in ARVD/C.
Conflict of interest statement
All other authors report no conflicts of interest.
Figures
Similar articles
-
Utility of tissue Doppler and strain echocardiography in arrhythmogenic right ventricular dysplasia/cardiomyopathy.Am J Cardiol. 2007 Aug 1;100(3):507-12. doi: 10.1016/j.amjcard.2007.03.053. Epub 2007 Jun 15. Am J Cardiol. 2007. PMID: 17659937
-
Evaluation of Structural Progression in Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy.JAMA Cardiol. 2017 Mar 1;2(3):293-302. doi: 10.1001/jamacardio.2016.5034. JAMA Cardiol. 2017. PMID: 28097316
-
Early detection of regional functional abnormalities in asymptomatic ARVD/C gene carriers.J Am Soc Echocardiogr. 2012 Sep;25(9):997-1006. doi: 10.1016/j.echo.2012.05.008. Epub 2012 Jun 21. J Am Soc Echocardiogr. 2012. PMID: 22727198
-
Current and future role of echocardiography in arrhythmogenic right ventricular dysplasia/cardiomyopathy.Cardiol J. 2015;22(4):362-74. doi: 10.5603/CJ.a2015.0018. Epub 2015 Mar 19. Cardiol J. 2015. PMID: 25786767 Review.
-
Noninvasive Multimodality Imaging in ARVD/C.JACC Cardiovasc Imaging. 2015 May;8(5):597-611. doi: 10.1016/j.jcmg.2015.02.007. JACC Cardiovasc Imaging. 2015. PMID: 25937197 Free PMC article. Review.
Cited by
-
Evaluation of Longitudinal Right Ventricular Mechanical Dyssynchrony before and Early after Cardiac Resynchronization Therapy: A Strain Imaging Study.J Tehran Heart Cent. 2011 Winter;6(1):24-30. Epub 2011 Feb 28. J Tehran Heart Cent. 2011. PMID: 23074601 Free PMC article.
-
A meta-analysis for echocardiographic assessment of right ventricular structure and function in ARVC.Echo Res Pract. 2016 Sep 29;3(3):95-104. doi: 10.1530/ERP-16-0028. Online ahead of print. Echo Res Pract. 2016. PMID: 27686556 Free PMC article.
-
Comprehensive multi-modality imaging approach in arrhythmogenic cardiomyopathy-an expert consensus document of the European Association of Cardiovascular Imaging.Eur Heart J Cardiovasc Imaging. 2017 Mar 1;18(3):237-253. doi: 10.1093/ehjci/jew229. Eur Heart J Cardiovasc Imaging. 2017. PMID: 28069601 Free PMC article. Review.
-
Right Ventricular Function in Arrhythmogenic Right Ventricular Cardiomyopathy: Potential Value of Strain Echocardiography.J Clin Med. 2024 Jan 26;13(3):717. doi: 10.3390/jcm13030717. J Clin Med. 2024. PMID: 38337410 Free PMC article. Review.
-
Scintigraphic spectrum of a patient population with suspected arrhythmogenic right ventricular dysplasia.Int J Cardiovasc Imaging. 2012 Jun;28(5):1267-77. doi: 10.1007/s10554-011-9918-y. Epub 2011 Jul 6. Int J Cardiovasc Imaging. 2012. PMID: 21732029
References
-
- Corrado D, Basso C, Thiene G, et al. Spectrum of clinicopathologic manifestations of arrhythmogenic right ventricular cardiomyopathy/dysplasia: a multicenter study. J Am Coll Cardiol. 1997;30:1512–20. - PubMed
-
- McKenna WJ, Thiene G, Nava A, et al. Diagnosis of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Task Force of the Working Group Myocardial and Pericardial Disease of the European Society of Cardiology and of the Scientific Council on Cardiomyopathies of the International Society and Federation of Cardiology. Br Heart J. 1994;71:215–8. - PMC - PubMed
-
- Kies P, Bootsma M, Bax J, Schalij MJ, van der Wall EE. Arrhythmogenic right ventricular dysplasia/cardiomyopathy: screening, diagnosis, and treatment. Heart Rhythm. 2006;3:225–34. - PubMed
-
- Dalal D, Nasir K, Bomma C, et al. Arrhythmogenic right ventricular dysplasia: a United States experience. Circulation. 2005;112:3823–32. - PubMed
-
- Hulot JS, Jouven X, Empana JP, Frank R, Fontaine G. Natural history and risk stratification of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Circulation. 2004;110:1879–84. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
