

A radiologic score to distinguish autoimmune hypophysitis from nonsecreting pituitary adenoma preoperatively
- PMID: 19628625
- PMCID: PMC7051493
- DOI: 10.3174/ajnr.A1714
A radiologic score to distinguish autoimmune hypophysitis from nonsecreting pituitary adenoma preoperatively
Abstract
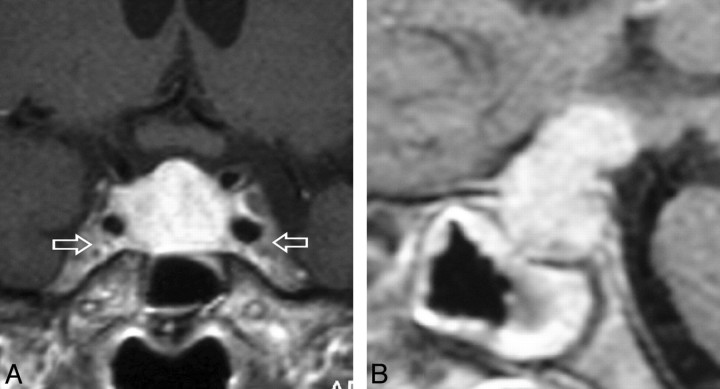
Background and purpose: Autoimmune hypophysitis (AH) mimics the more common nonsecreting pituitary adenomas and can be diagnosed with certainty only histologically. Approximately 40% of patients with AH are still misdiagnosed as having pituitary macroadenoma and undergo unnecessary surgery. MR imaging is currently the best noninvasive diagnostic tool to differentiate AH from nonsecreting adenomas, though no single radiologic sign is diagnostically accurate. The purpose of this study was to develop a scoring system that summarizes numerous MR imaging signs to increase the probability of diagnosing AH before surgery.
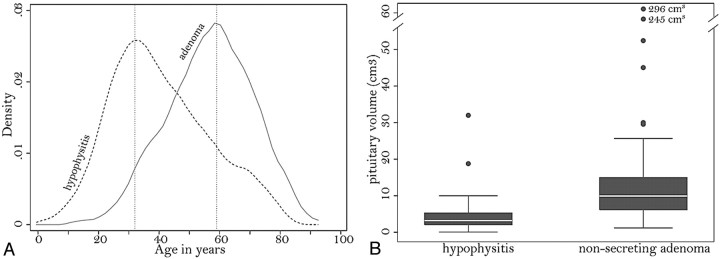
Materials and methods: This was a case-control study of 402 patients, which compared the presurgical pituitary MR imaging features of patients with nonsecreting pituitary adenoma and controls with AH. MR images were compared on the basis of 16 morphologic features besides sex, age, and relation to pregnancy.
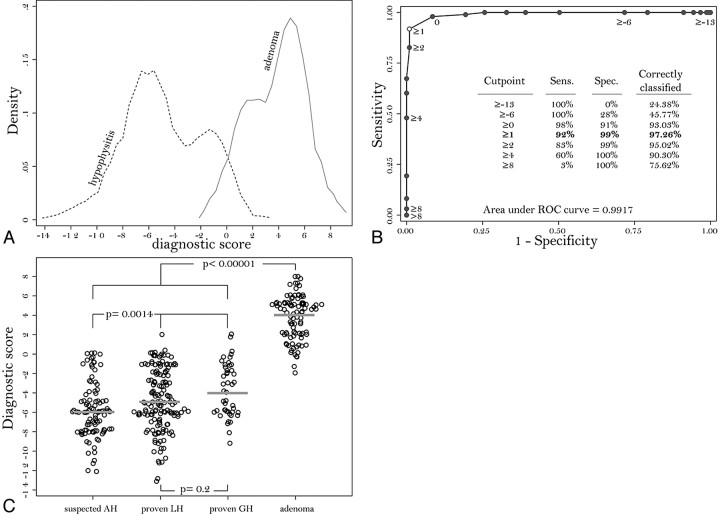
Results: Only 2 of the 19 proposed features tested lacked prognostic value. When the other 17 predictors were analyzed jointly in a multiple logistic regression model, 8 (relation to pregnancy, pituitary mass volume and symmetry, signal intensity and signal intensity homogeneity after gadolinium administration, posterior pituitary bright spot presence, stalk size, and mucosal swelling) remained significant predictors of a correct classification. The diagnostic score had a global performance of 0.9917 and correctly classified 97% of the patients, with a sensitivity of 92%, a specificity of 99%, a positive predictive value of 97%, and a negative predictive value of 97% for the diagnosis of AH.
Conclusions: This new radiologic score could be integrated into the management of patients with AH, who derive greater benefit from medical as opposed to surgical treatment.
Figures
References
-
- Daly AF, Rixhon M, Adam C, et al. High prevalence of pituitary adenomas: a cross-sectional study in the province of Liege, Belgium. J Clin Endocrinol Metab 2006;91:4769–75. Epub 2006 Sep 12 - PubMed
-
- Ezzat S, Asa SL, Couldwell WT, et al. The prevalence of pituitary adenomas: a systematic review. Cancer 2004;101:613–19 - PubMed
-
- Biller BM, Swearingen B, Zervas NT, et al. A decade of the Massachusetts General Hospital Neuroendocrine Clinical Center. J Clin Endocrinol Metab 1997;82:1668–74 - PubMed
-
- Chanson P, Brochier S. Non-functioning pituitary adenomas. J Endocrinol Invest 2005;28:93–99 - PubMed
-
- Asa SL. Practical pituitary pathology: what does the pathologist need to know? Arch Pathol Lab Med 2008;132:1231–40 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical