

Aicardi-Goutieres syndrome: neuroradiologic findings and follow-up
- PMID: 19628626
- PMCID: PMC7051307
- DOI: 10.3174/ajnr.A1694
Aicardi-Goutieres syndrome: neuroradiologic findings and follow-up
Abstract
Background and purpose: To date, few studies have focused specifically on imaging findings in Aicardi-Goutières syndrome (AGS). We set out to evaluate retrospectively neuroradiologic data from a large sample of patients with AGS, focusing on the pattern of white matter abnormalities and the temporal evolution of the cerebral involvement to establish the radiologic natural history of the disease.
Materials and methods: Thirty-six patients, 18 girls and 18 boys, were included. All had a clinical diagnosis of AGS, genetically confirmed in 31 of them. For every subject, we reviewed at least 1 CT and 1 MR imaging study; 19 (52.7%) had multiple examinations. In all, we reviewed 109 examinations. Clinical-neuroradiologic comparisons were analyzed by using the chi(2) test.
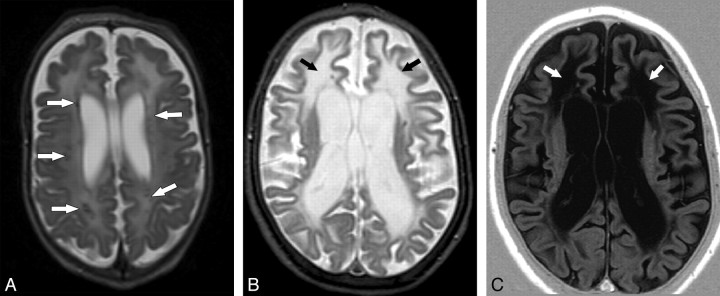
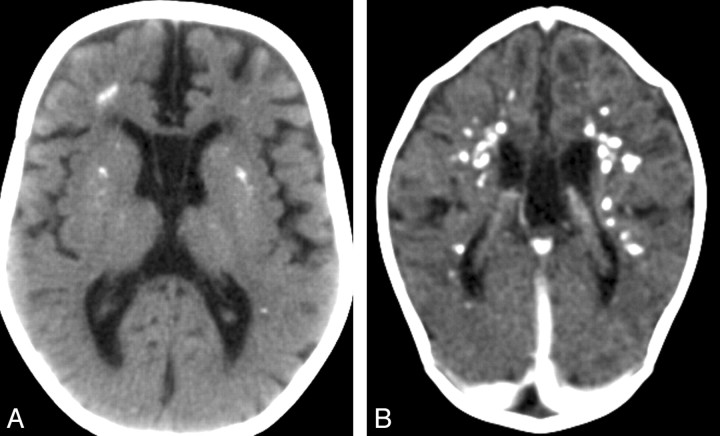
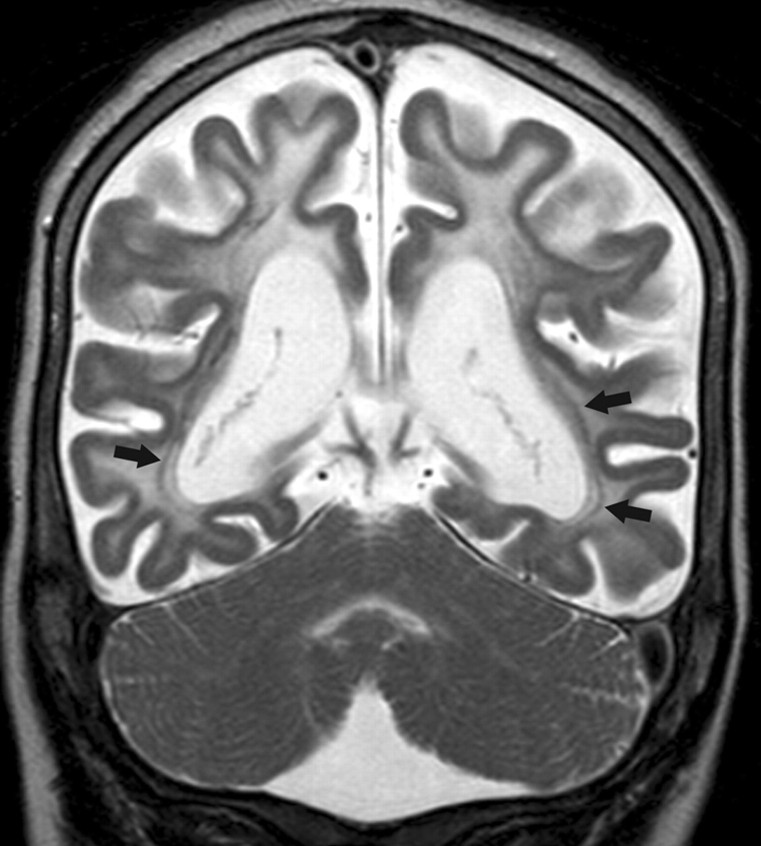
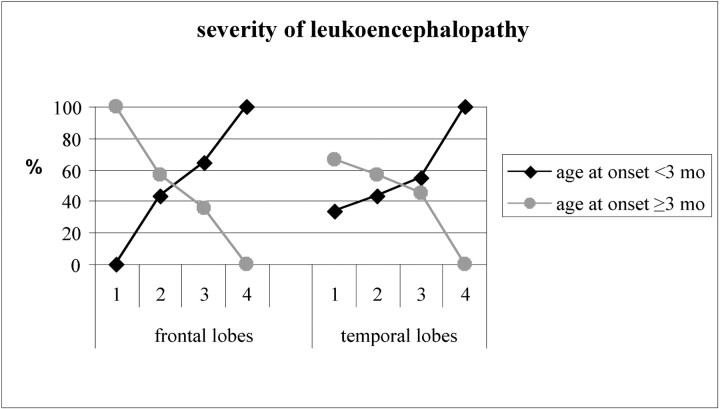
Results: Calcifications were found in all subjects, mainly in the basal ganglia, lobar white matter, and dentate nuclei. Abnormal white matter was present in all the subjects, showing 2 patterns of distribution: diffuse in 18 (50%) and an anteroposterior gradient in 18 (50%). Cystic areas were observed in the temporal and/or frontal lobes in 12/36 patients (33.3%). A correlation was found between early age at onset and severity of the leukoencephalopathy in the frontal (P = .024) and temporal (P = .034) regions. A significant degree of cerebral atrophy was found in 31/36 subjects (86.1%). The neuroradiologic presentation remained substantially stable with time.
Conclusions: The different neuroradiologic presentations of AGS are here outlined for the first time in a large sample of patients. These findings may facilitate more precise and earlier diagnosis of this rare but probably underdiagnosed syndrome.
Figures
Comment in
-
Reconciling neuroimaging and clinical findings in Aicardi-Goutières syndrome: an autoimmune-mediated encephalopathy.AJNR Am J Neuroradiol. 2010 Aug;31(7):E62-3; author reply E64. doi: 10.3174/ajnr.A2147. Epub 2010 Jun 25. AJNR Am J Neuroradiol. 2010. PMID: 20581073 Free PMC article. No abstract available.
References
-
- Aicardi J, Goutières F. A progressive familial encephalopathy in infancy with calcifications of the basal ganglia and chronic cerebrospinal fluid lymphocytosis. Ann Neurol 1984;15:49–54 - PubMed
-
- Goutières F, Aicardi J, Barth PG, et al. Aicardi–Goutières syndrome: an update and results of interferon-alpha studies. Ann Neurol 1998;44:900–07 - PubMed
-
- Lanzi G, Fazzi E, D'Arrigo S, et al. The natural history of Aicardi–Goutières syndrome: follow-up of 11 Italian patients. Neurology 2005;64:1621–24 - PubMed
-
- Goutières F. Aicardi-Goutières syndrome. Brain Dev 2005;27:201–06 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical