

Risk factors for cyclosporin A nephrotoxicity in children with steroid-dependant nephrotic syndrome
- PMID: 19628686
- PMCID: PMC2736699
- DOI: 10.2215/CJN.01520209
Risk factors for cyclosporin A nephrotoxicity in children with steroid-dependant nephrotic syndrome
Abstract
Background and objectives: Cyclosporin A (CsA) is a well-established treatment for steroid-dependent nephrotic syndrome (SDNS) that may, however, cause chronic ischemic renal lesions. The objective of the study was to assess the prevalence of CsA nephrotoxicity (CsAN) in protocol biopsies of children with SDNS.
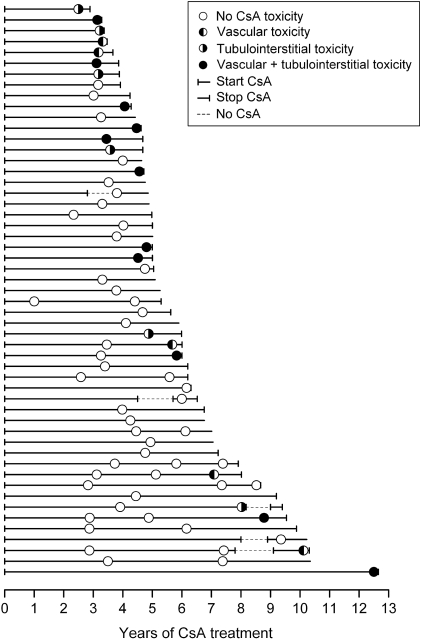
Design, settings, participants, & measurements: From 1990 through 2008, we performed 71 renal biopsies in 53 patients with SDNS. The mean CsA C2 levels were 466 +/- 134 ng/ml, and the mean duration of treatment was 4.7 +/- 2.0 yr before biopsy (range 2.9 to 12.7 yr).
Results: CsAN was observed in 22 (31%) of 71 renal biopsies. Of these, 11 corresponded to isolated vascular or tubular lesions, and 11 corresponded to combined vascular and tubular lesions. The majority of CsAN lesions were mild (17 of 22). In no cases were lesions graded as severe. By regression analysis, CsAN was positively associated with the use of angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin II receptor blockers (ARBs) and with hyperuricemia and negatively associated with minimal-change lesions. By multivariate analysis, only association with the use of ACEIs or ARBs retained significance. Stratification of the population according to CsA C2 levels showed increased risk for CsAN for C2 levels >600 ng/ml.
Conclusions: Mild to moderate CsAN occurs in approximately one third of patients who have SDNS and are treated with CsA for >3 yr. Our data suggest that patients who require high dosages of CsA or treatment for hypertension, in particular when ACEIs/ARBs are used, are at higher risk for CsAN.
Figures

References
-
- Niaudet P, Habib R, Tete MJ, Hinglais N, Broyer M: Cyclosporin in the treatment of idiopathic nephrotic syndrome in children. Pediatr Nephrol 1: 566–573, 1987 - PubMed
-
- Hodson EM, Willis NS, Craig JC: Non-corticosteroid treatment for nephrotic syndrome in children. Cochrane Database Syst Rev (23): CD002290, 2008 - PubMed
-
- Ehrich JH, Geerlings C, Zivicnjak M, Franke D, Geerlings H, Gellermann J: Steroid-resistant idiopathic childhood nephrosis: Overdiagnosed and undertreated. Nephrol Dial Transplant 22: 2183–2193, 2007 - PubMed
-
- Niaudet P, Habib R: Cyclosporine in the treatment of idiopathic nephrosis. J Am Soc Nephrol 5: 1049–1056, 1994 - PubMed
-
- Mathieson PW: Proteinuria and immunity: An overstated relationship? N Engl J Med 359: 2492–2494, 2008 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
