

Diagnosis and treatment of vertigo and dizziness
- PMID: 19629221
- PMCID: PMC2696792
- DOI: 10.3238/arztebl.2008.0173
Diagnosis and treatment of vertigo and dizziness
Abstract
Introduction: Vertigo is not a separate disease process, but a multisensory and sensorimotor syndrome with various etiologies and pathogeneses. It is among the commonest symptoms presented to doctors, with a lifetime prevalence of around 20% to 30%. Patients have often consulted multiple physicians before a diagnosis is made and therapy initiated.
Methods: Selective literature research and review of the guidelines of the German Neurological Society.
Results: A careful history remains the cornerstone of diagnosis. Once the correct diagnosis is made, specific and effective treatments are available for most peripheral, central, and psychogenic forms of dizziness. Treatment may include medication, physiotherapy, and psychotherapy; a few limited cases may require surgical treatment. The treatment of choice for acute vestibular neuritis is the administration of corticosteroids. Menière's disease is treated with high-dose, long-term betahistine. A new approach to the management of downbeat and upbeat nystagmus, and of episodic ataxia type 2, involves the use of aminopyridines as potassium-channel blockers. Close multidisciplinary cooperation is essential in dizziness, and further multicenter studies are needed.
Keywords: Menière’s disease; dizziness; migraine; presenting complaint; vertigo; vestibular disorder.
Figures
References
-
- Neuhauser HK. Epidemiology of vertigo. Curr Opin Neurol. 2007;20:40–46. - PubMed
-
- Brandt T, Dieterich M, Strupp M. Vertigo - Leitsymptom Schwindel. Darmstadt: Steinkopff; 2003.
-
- Karlberg M, Hall K, Quickert N, Hinson J, Halmagyi GM. What inner ear diseases cause benign paroxysmal positional vertigo? Acta Otolaryngol. 2000;120:380–385. - PubMed
-
- Brandt T, Steddin S. Current view of the mechanism of benign paroxysmal positioning vertigo: cupulolithiasis or canalolithiasis? J Vestib Res. 1993;3:373–382. - PubMed
-
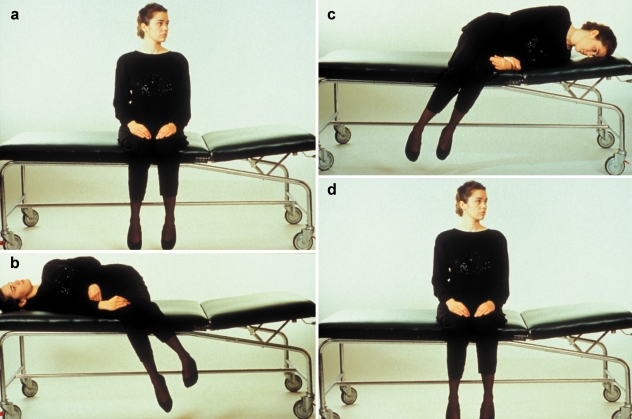
- Semont A, Freyss G, Vitte E. Curing the BPPV with a liberatory maneuver. Adv Otorhinolaryngol. 1988;42:290–293. - PubMed
LinkOut - more resources
Full Text Sources
Medical