

Sonographic evaluation of vessel grafts in living donor liver transplantation recipients of the right lobe
- PMID: 19630113
- PMCID: PMC2715984
- DOI: 10.3748/wjg.15.3550
Sonographic evaluation of vessel grafts in living donor liver transplantation recipients of the right lobe
Abstract
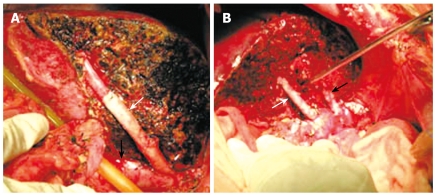
Aim: To evaluate the vessel grafts (VG) used to reconstruct the middle hepatic vein (MHV) tributaries with ultrasonography.
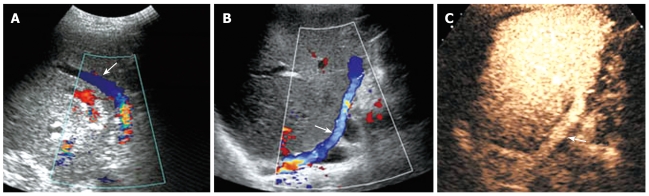
Methods: Twenty-four patients undergone living donor liver transplantation were enrolled in our study. MHV tributaries larger than 5 mm in diameter were reconstructed with interposition VG. Blood flow of the graft and interposition VG was checked by Doppler ultrasonography daily in the first 2 postoperative weeks and monthly followed up after discharge. The sensitivity of VG detected by ultrasonography was assessed using surgical records as references. Student's t test was used to compare the velocity of VG and occluded VG in chronic patents (> 3 mo).
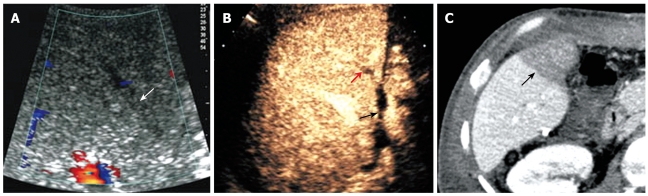
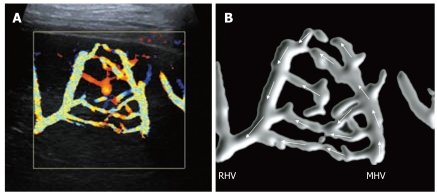
Results: Thirty-one VG were used to reconstruct the MHV tributaries. Ultrasonography identified 96.7% (30/31) of large MHV tributaries and 90.3% (28/31) of VG. The diameter of VG was 5.6 +/- 0.8 mm and the velocity of VG was 19.7 +/- 8.1 cm/s. Two VG (2/31, 6.5%) were occluded on the first postoperative day in one patient who suffered from persistent ascites and had a prolonged recovery of liver function. Twenty-six VG (26/31, 83.9%) were patent 2 wk after operation. Six (6/31, 19.4%) VG were patent over 3 mo after operation. Intrahepatic venous collaterals were detected in 29.2% (7/24) patients. The velocity of VG and occluded VG was 30.1 +/- 5.6 cm/s, 16.5 +/- 5.8 cm/s, respectively, in chronic patents. The difference between two groups was statistically significant (P < 0.001).
Conclusion: Our results indicate that most VG are patent in the first postoperative week while only a small portion with a higher velocity remains patent after 3 mo. Intrahepatic venous collaterals can be observed in some patients after occlusion of VG.
Figures
Similar articles
-
Intrahepatic venous collaterals formation following outflow block in adult-to-adult living donor liver transplantation.J Surg Res. 2008 May 15;146(2):172-6. doi: 10.1016/j.jss.2007.05.017. Epub 2007 Dec 26. J Surg Res. 2008. PMID: 18155251
-
Doppler sonographic abnormalities suggestive of venous congestion in the right lobe graft of living donor liver transplant recipients.AJR Am J Roentgenol. 2007 Mar;188(3):W239-45. doi: 10.2214/AJR.05.1761. AJR Am J Roentgenol. 2007. PMID: 17312029 Review.
-
Doppler sonography to diagnose venous congestion in a modified right lobe graft after living donor liver transplantation.AJR Am J Roentgenol. 2008 Apr;190(4):1010-7. doi: 10.2214/AJR.07.2825. AJR Am J Roentgenol. 2008. PMID: 18356449
-
Modified right liver graft from a living donor to prevent congestion.Transplantation. 2002 Jul 15;74(1):54-9. doi: 10.1097/00007890-200207150-00010. Transplantation. 2002. PMID: 12134099 Clinical Trial.
-
Management of the middle hepatic vein and its tributaries in right lobe living donor liver transplantation.Hepatobiliary Pancreat Dis Int. 2007 Aug;6(4):358-63. Hepatobiliary Pancreat Dis Int. 2007. PMID: 17690029 Review.
References
-
- Trotter JF, Wachs M, Everson GT, Kam I. Adult-to-adult transplantation of the right hepatic lobe from a living donor. N Engl J Med. 2002;346:1074–1082. - PubMed
-
- Inomata Y, Uemoto S, Asonuma K, Egawa H. Right lobe graft in living donor liver transplantation. Transplantation. 2000;69:258–264. - PubMed
-
- Kim BW, Park YK, Paik OJ, Lee BM, Wang HJ, Kim MW. Effective anatomic reconstruction of the middle hepatic vein in modified right lobe graft living donor liver transplantation. Transplant Proc. 2007;39:3228–3233. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
