

Risk stratification for sudden cardiac death: is there a clinical role for T wave alternans?
- PMID: 19631909
- PMCID: PMC2761079
- DOI: 10.1016/j.hrthm.2009.05.025
Risk stratification for sudden cardiac death: is there a clinical role for T wave alternans?
Abstract
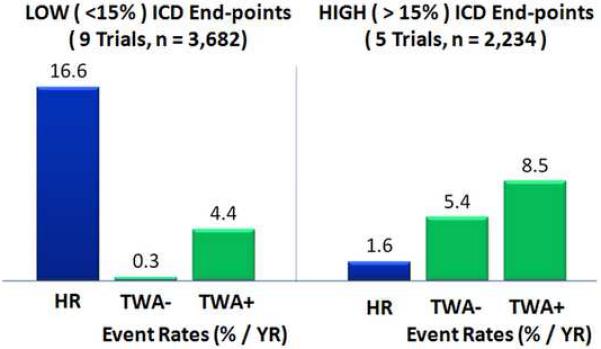
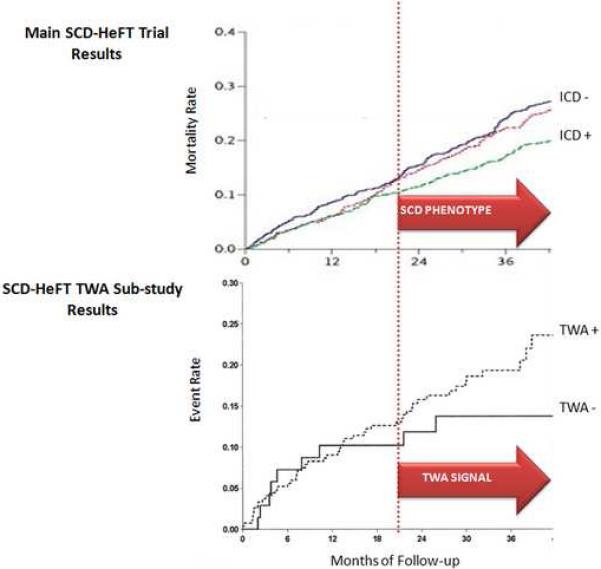
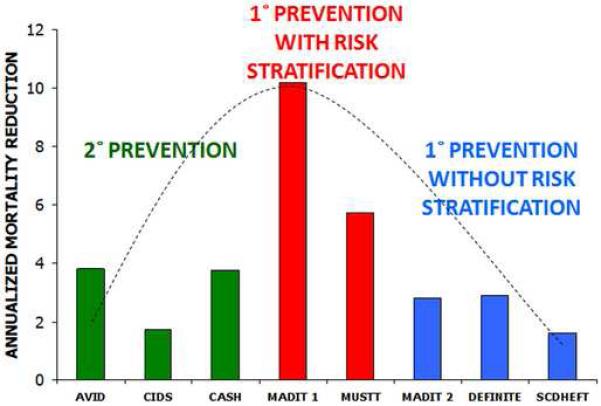
The proportion of cardiovascular deaths attributable to sudden cardiac death (SCD) is on the rise. Herein lies the rationale for developing risk stratification strategies to predict who will benefit from prophylactic implantable cardioverter-defibrillator (ICD) implantation. Current guidelines recommend prophylactic ICD therapy in patients with reduced left ventricular ejection fraction (LVEF). However, there are clear limitations in using LVEF alone to decide who should receive an ICD. There is mounting evidence that microvolt-level T-wave alternans (TWA) is an important marker of arrhythmic risk. TWA is appealing because it noninvasively probes the underlying electrophysiological substrate and has been linked to cellular mechanisms for arrhythmias. This review considers the clinical role of TWA for risk stratification of SCD.
Figures

Similar articles
-
Microvolt T-wave alternans for the risk stratification of dangerous ventricular arrhythmias in patients with previously implanted automatic cardioverter-defibrillator.Kardiol Pol. 2011;69(6):580-5. Kardiol Pol. 2011. PMID: 21678296
-
Lack of Prognostic Value of T-Wave Alternans for Implantable Cardioverter-Defibrillator Benefit in Primary Prevention.J Am Heart Assoc. 2024 Jun 4;13(11):e032465. doi: 10.1161/JAHA.123.032465. Epub 2024 May 28. J Am Heart Assoc. 2024. PMID: 38804218 Free PMC article.
-
Role of microvolt T-wave alternans in assessment of arrhythmia vulnerability among patients with heart failure and systolic dysfunction: primary results from the T-wave alternans sudden cardiac death in heart failure trial substudy.Circulation. 2008 Nov 11;118(20):2022-8. doi: 10.1161/CIRCULATIONAHA.107.748962. Epub 2008 Oct 27. Circulation. 2008. PMID: 18955671 Free PMC article. Clinical Trial.
-
Risk stratification after myocardial infarction: is left ventricular ejection fraction enough to prevent sudden cardiac death?Eur Heart J. 2013 Jul;34(26):1964-71. doi: 10.1093/eurheartj/eht109. Epub 2013 May 3. Eur Heart J. 2013. PMID: 23644180 Review.
-
Utility of microvolt T-wave alternans to predict sudden cardiac death in patients with cardiomyopathy.Curr Opin Cardiol. 2007 Jan;22(1):25-32. doi: 10.1097/HCO.0b013e328011aa49. Curr Opin Cardiol. 2007. PMID: 17143041 Review.
Cited by
-
Minimizing repolarization-related proarrhythmic risk in drug development and clinical practice.Drugs. 2010 Mar 26;70(5):573-603. doi: 10.2165/11535230-000000000-00000. Drugs. 2010. PMID: 20329805 Review.
-
In Vivo and In Silico Investigation Into Mechanisms of Frequency Dependence of Repolarization Alternans in Human Ventricular Cardiomyocytes.Circ Res. 2016 Jan 22;118(2):266-78. doi: 10.1161/CIRCRESAHA.115.307836. Epub 2015 Nov 24. Circ Res. 2016. PMID: 26602864 Free PMC article.
-
T-wave alternans and ST depression assessment identifies low risk individuals with ischemic cardiomyopathy in the absence of left ventricular hypertrophy.Ann Noninvasive Electrocardiol. 2013 Jul;18(4):359-68. doi: 10.1111/anec.12051. Epub 2013 May 3. Ann Noninvasive Electrocardiol. 2013. PMID: 23879276 Free PMC article.
-
Role of substrate and triggers in the genesis of cardiac alternans, from the myocyte to the whole heart: implications for therapy.Circulation. 2012 Jan 24;125(3):539-49. doi: 10.1161/CIRCULATIONAHA.111.033563. Circulation. 2012. PMID: 22271847 Free PMC article. Review. No abstract available.
-
Novel algorithm for identifying T-wave current density alternans using synthesized 187-channel vector-projected body surface mapping.Heart Vessels. 2011 Mar;26(2):160-7. doi: 10.1007/s00380-010-0042-z. Epub 2010 Oct 30. Heart Vessels. 2011. PMID: 21052691
References
-
- Bardy GH, Lee KL, Mark DB, Poole JE, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–37. - PubMed
-
- Bloomfield DM, Bigger JT, Steinman RC, et al. Microvolt T-wave alternans and the risk of death or sustained ventricular arrhythmias in patients with left ventricular dysfunction. J Am Coll Cardiol. 2006;47:456–63. - PubMed
-
- Bloomfield DM, Steinman RC, Namerow PB, et al. Microvolt T-wave alternans distinguishes between patients likely and patients not likely to benefit from implanted cardiac defibrillator therapy: a solution to the Multicenter Automatic Defibrillator Implantation Trial (MADIT) II conundrum. Circulation. 2004;110:1885–9. - PubMed
-
- Buxton AE. Should everyone with an ejection fraction less than or equal to 30% receive an implantable cardioverter-defibrillator? Not everyone with an ejection fraction < or = 30% should receive an implantable cardioverter-defibrillator. Circulation. 2005;111:2537–49. discussion 2537-49. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
