

CR represents an early index of potential long survival in multiple myeloma
- PMID: 19633690
- PMCID: PMC5777472
- DOI: 10.1038/bmt.2009.176
CR represents an early index of potential long survival in multiple myeloma
Abstract
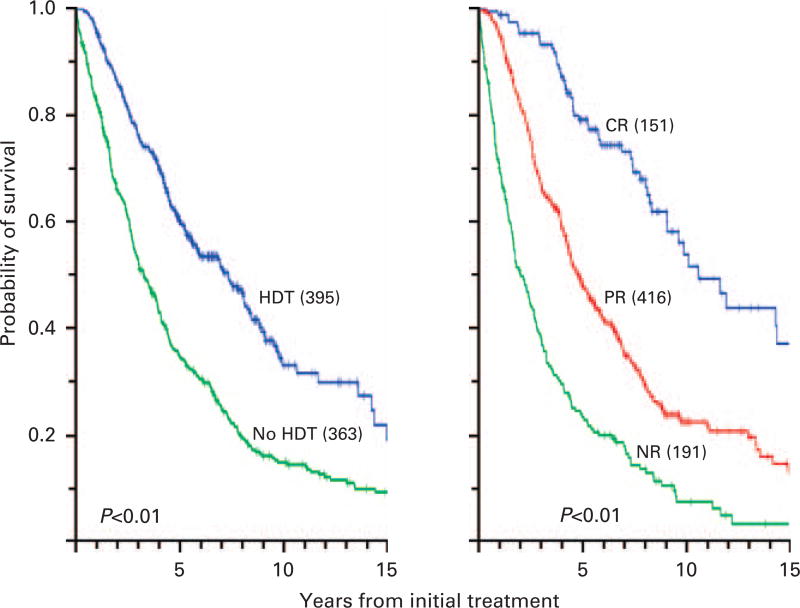
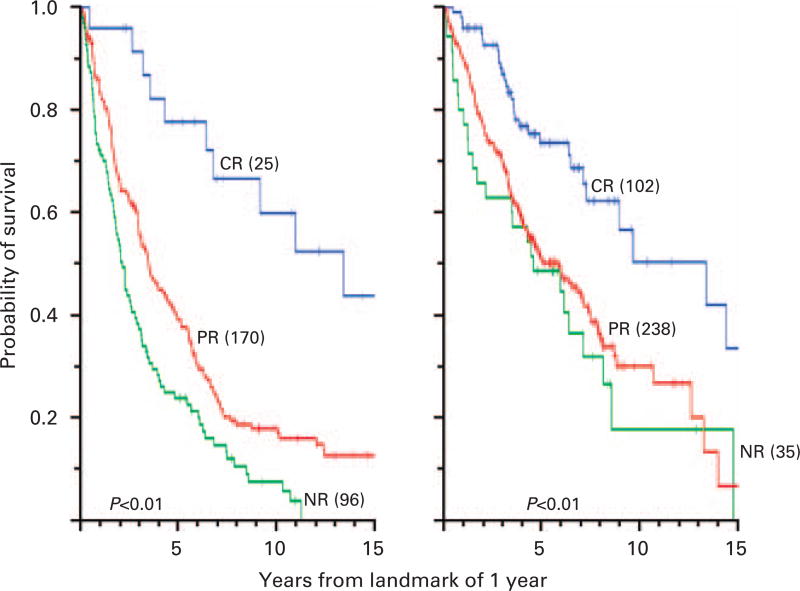
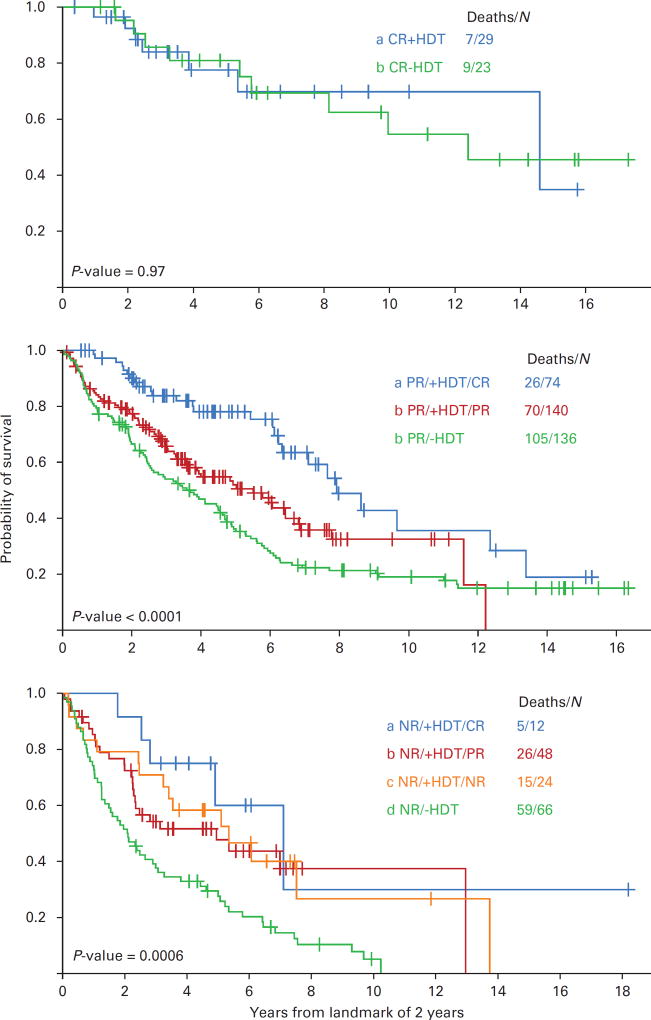
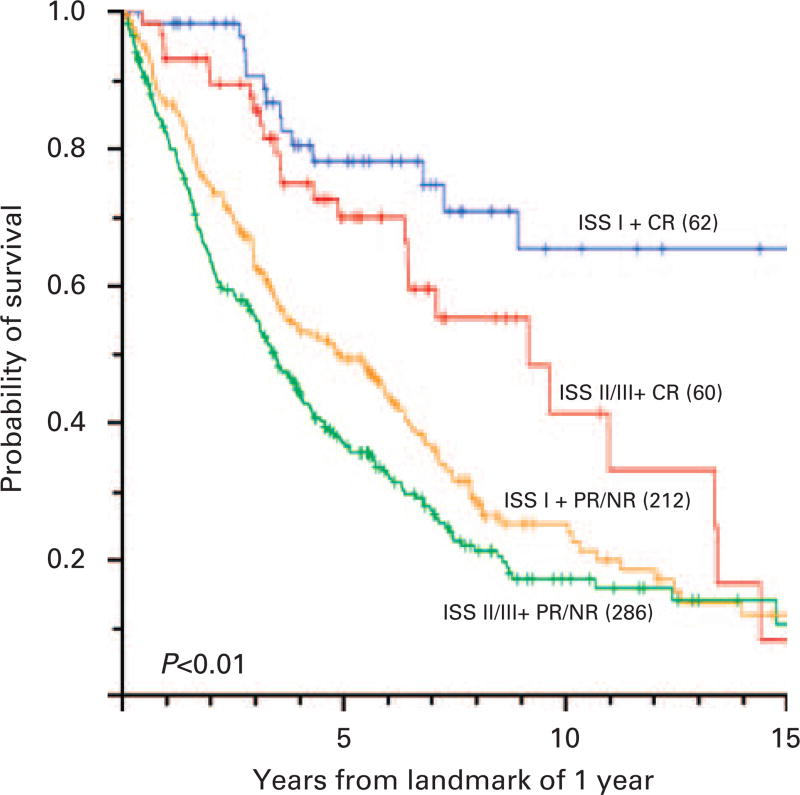
To assess the impact of CR on survival in multiple myeloma. Retrospective evaluation of response and survival among 758 consecutive patients with multiple myeloma treated at a single center, of whom 395 patients received intensive therapy supported by autologous stem cells within the first year. Survival times were calculated after 1 and 2 years from the start of chemotherapy. On the basis of the response status after a 2-year landmark, the subsequent median survival was 9.7 years for patients with CR, 4.4 years for those with PR and 2.7 years for patients with NR (P<0.001). Longer survival was attributed in part to intensive therapy that converted the myeloma of 67% of patients with NR to PR or CR, and induced CR in 26% of patients with PR. Intensive therapy did not prolong survival for patients with CR after primary therapy. For patients with multiple myeloma, Cox regression analyses showed that CR was the dominant prognostic factor for long survival, followed by stage I disease, PR and intensive treatment as independent factors. A cure fraction of 2% was identified for nine patients who have remained in CR >10 years.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Attal M, Harousseau JL, Stoppa AM, Sotto JJ, Fuzibet JG, Rossi JF, et al. A prospective, randomized trial of autologous bone marrow transplantation and chemotherapy in multiple myeloma. N Engl J Med. 1996;335:91–97. - PubMed
-
- Child J, Morgan G, Davies F, Owen R, Bell S, Hawkins K, et al. High-dose chemotherapy with hematopoietic stem-cell rescue for multiple myeloma. N Engl J Med. 2003;348:1875–1883. - PubMed
-
- Alexanian R, Barlogie B, Tucker S. VAD-based regimens as primary treatment for multiple myeloma. Am J Hematol. 1990;33:86–89. - PubMed
-
- Alexanian R, Dimopoulos M, Delasalle K, Barlogie B. Primary dexamethasone treatment of multiple myeloma. Blood. 1992;80:887–890. - PubMed
-
- Weber D, Rankin K, Gavino M, Delasalle K, Alexanian R. Thalidomide alone or with dexamethasone for previously untreated multiple myeloma. J Clin Oncol. 2003;21:16–19. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
