

Conditional and continuous electrical stimulation increase cystometric capacity in persons with spinal cord injury
- PMID: 19634166
- PMCID: PMC3109497
- DOI: 10.1002/nau.20766
Conditional and continuous electrical stimulation increase cystometric capacity in persons with spinal cord injury
Abstract
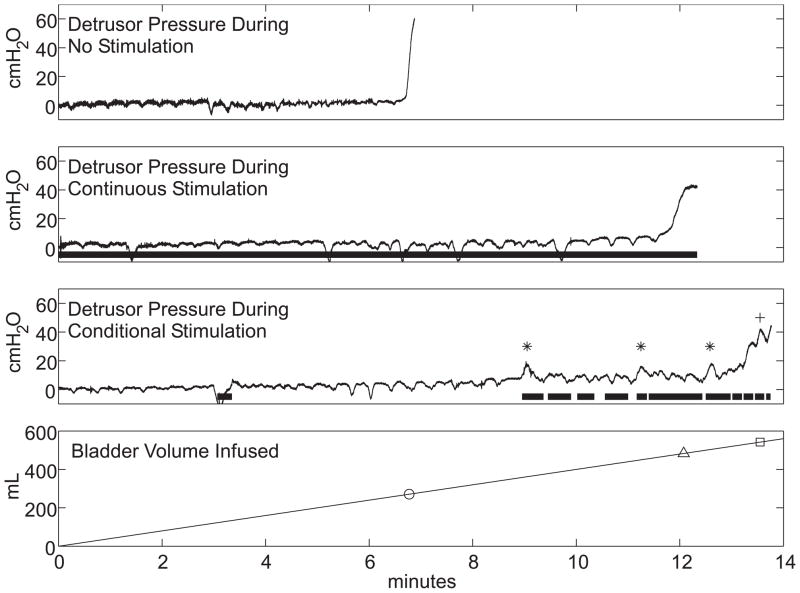
Aims: Individuals with spinal cord injury (SCI) exhibit neurogenic detrusor overactivity (NDO) causing high intravesicle pressures and incontinence. The first aim was to measure changes in maximum cystometric capacity (MCC) evoked by electrical stimulation of the dorsal genital nerve (DGN) delivered either continuously or conditionally (only during bladder contractions) in persons with SCI. The second aim was to use the external anal sphincter electromyogram (EMG(EAS)) for real-time control of conditional stimulation.
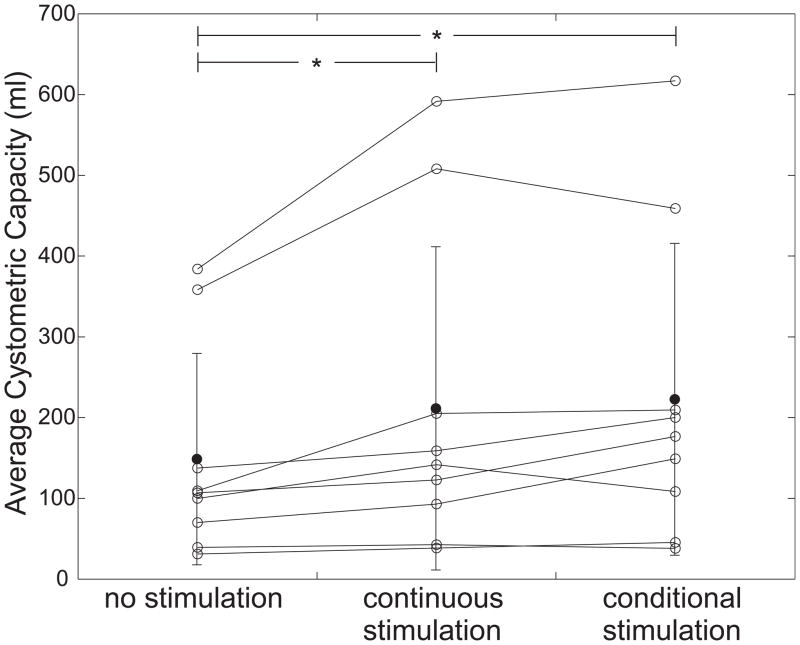
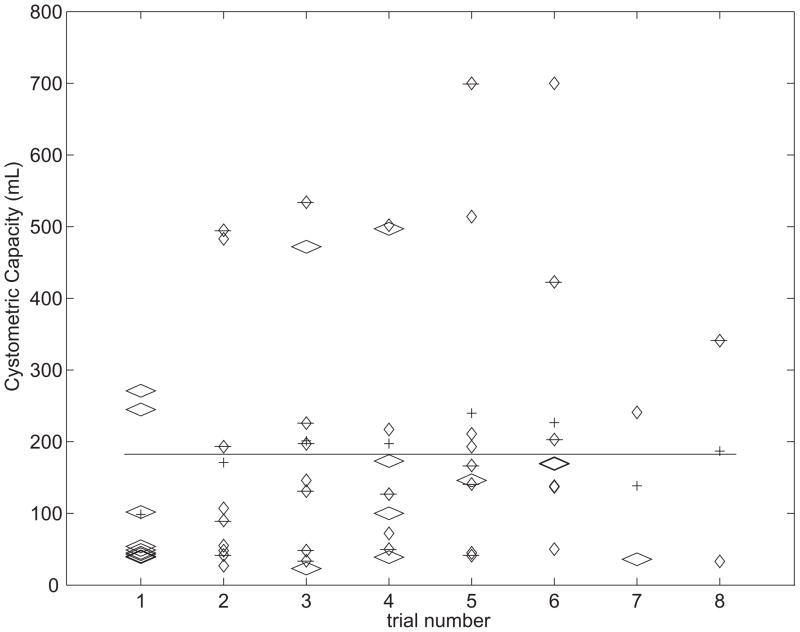
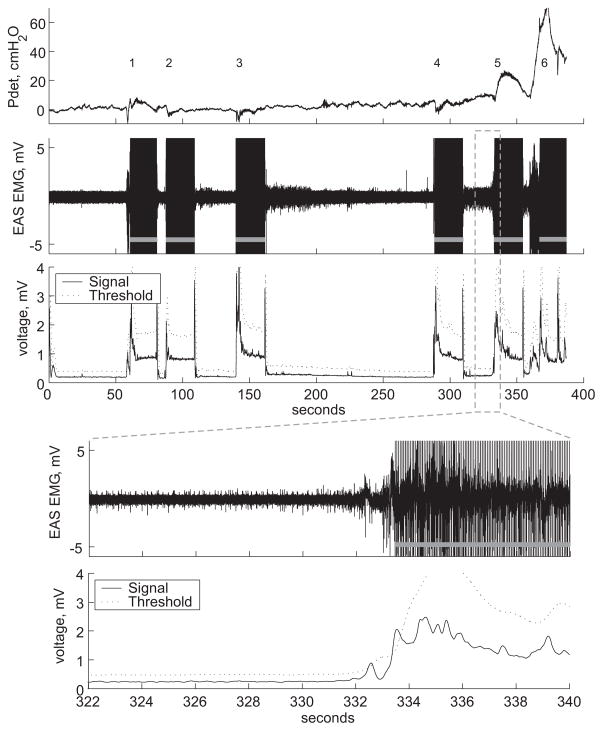
Methods: Serial filling cystometries were performed in nine volunteers with complete or incomplete supra-sacral SCI. Conditional stimulation was delivered automatically when detrusor pressure increased to 8-12 cmH(2)O above baseline. MCCs were measured for each treatment (continuous, conditional, and no stimulation) and compared using post-ANOVA Tukey HSD paired comparisons. Additional treatments in two subjects used the EMG(EAS) for automatic control of conditional stimulation.
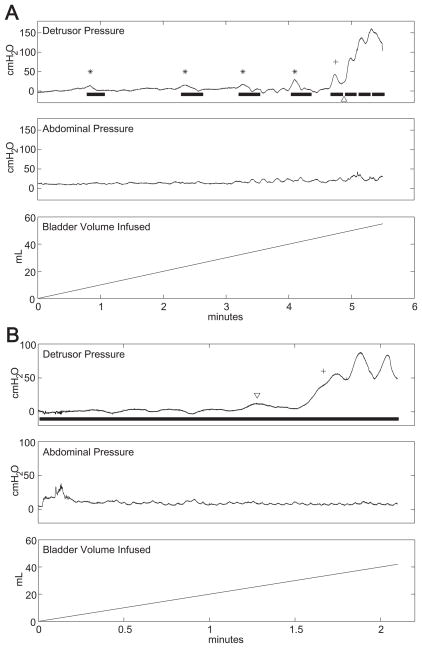
Results: Continuous and conditional stimulation increased MCC by 63 +/- 73 ml (36 +/- 24%) and 74 +/- 71 ml (51 +/- 37%), respectively (P < 0.05), compared to no stimulation. There was no significant difference between MCCs for conditional and continuous stimulation, but conditional stimulation significantly reduced stimulation time (174 +/- 154 sec, or 27 +/- 17% of total time) as compared to continuous stimulation (469 +/- 269 sec, 100% of total time, P < 0.001). The EMG(EAS) algorithm provided reliable detection of bladder contractions (six of six contractions over four trials) and reduced stimulation time (21 +/- 8% of total time).
Conclusions: Conditional stimulation generates increases in bladder capacity while substantially reducing stimulation time. Furthermore, EMG(EAS) was successfully used as a real-time feedback signal to control conditional electrical stimulation in a laboratory setting.
(c) 2009 Wiley-Liss, Inc.
Figures
References
-
- Shingleton WB, Bodner DR. The development of urologic complications in relationship to bladder pressure in spinal cord injured patients. J Am Paraplegia Soc. 1993;16:14–17. - PubMed
-
- Watanabe T, Rivas DA, Chancellor MB. Urodynamics of spinal cord injury. Urol Clin North Am. 1996;23:459–473. - PubMed
-
- Petersen T, Nielsen JB, Schroder HD. Intravesical capsaicin in patients with detrusor hyper-reflexia--a placebo-controlled cross-over study. Scand J Urol Nephrol. 1999;33:104–110. - PubMed
-
- Schurch B. What is new in detrusor-sphincter dyssynergia treatment in spinal cord injury patients? NeuroRehabilitation. 1998;10:267–279.
-
- Staskin DR. Hydroureteronephrosis after spinal cord injury. Effects of lower urinary tract dysfunction on upper tract anatomy. Urol Clin North Am. 1991;18:309–316. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
