

Pancreatic cancer related cachexia: influence on metabolism and correlation to weight loss and pulmonary function
- PMID: 19635171
- PMCID: PMC2741486
- DOI: 10.1186/1471-2407-9-255
Pancreatic cancer related cachexia: influence on metabolism and correlation to weight loss and pulmonary function
Abstract
Background: Dramatic weight loss is an often underestimated symptom in pancreatic cancer patients. Cachexia- defined as an unintended loss of stable weight exceeding 10%--is present in up to 80% of patients with cancer of the upper gastrointestinal tract, and has a significant influence on survival. The aim of the study was to show the multiple systemic effects of cachexia in pancreatic cancer patients, in terms of resection rate, effects on pulmonary function, amount of fat and muscle tissue, as well as changes in laboratory parameters.
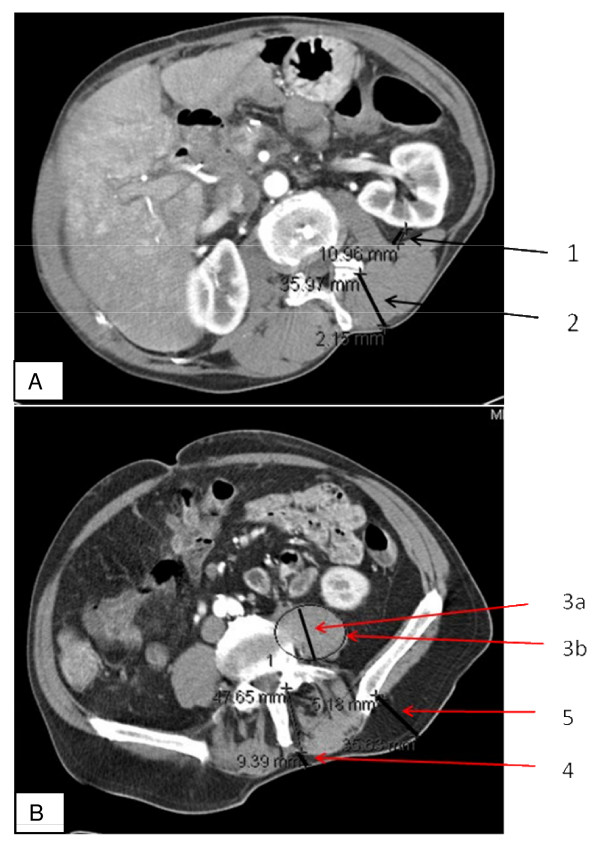
Methods: In patients with pancreatic cancer, clinical appearance was documented, including the amount of weight loss. Laboratory parameters and lung-function tests were evaluated, and the thickness of muscle and fat tissue was measured with computed tomography scans. Statistical analysis, including multivariate analysis, was performed using SPSS software. Survival curves were calculated using Kaplan-Meier analysis and the log-rank test. To test for significant differences between the examined groups we used Student's t-test and the Mann-Whitney U test. Significance was defined as p < 0.05.
Results: Of 198 patients with a ductal adenocarcinoma of the pancreas, 70% were suffering from weight loss when they presented for operation, and in 40% weight loss exceeded 10% of the stable weight. In patients with cachexia, metastases were diagnosed significantly more often (47% vs. 24%, P < 0.001), leading to a significantly reduced resection rate in these patients. Patients with cachexia had significantly reduced fat tissue amounts. Hence, dramatic weight loss in a patient with pancreatic cancer may be a hint of a more progressed or more aggressive tumour.
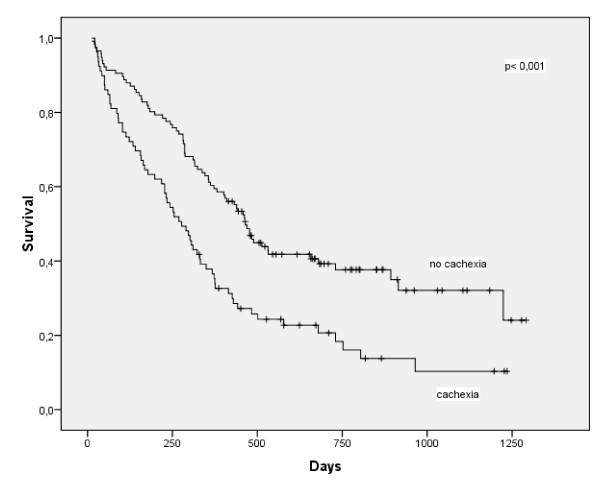
Conclusion: Pancreatic cancer patients with cachexia had a higher rate of more progressed tumour stages and a worse nutritional status. Furthermore, patients with cachexia had an impaired lung function and a reduction in fat tissue. Patients with pancreatic cancer and cachexia had significantly reduced survival. If weight loss exceeded 5% there was a significantly reduced resection rate to detect, but the changes were significantly more substantial if weight loss was 10% or more. We propose that a weight loss of 10% be defined as significant in pancreatic cancer.
Figures
References
-
- Friess H, Isenmann R, Berberat P, Kleeff J, Buchler MW. [Prognosis in pancreatic carcinoma] Ther Umsch. 1996;53(5):401–407. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
