

Myocyte necrosis underlies progressive myocardial dystrophy in mouse dsg2-related arrhythmogenic right ventricular cardiomyopathy
- PMID: 19635863
- PMCID: PMC2722163
- DOI: 10.1084/jem.20090641
Myocyte necrosis underlies progressive myocardial dystrophy in mouse dsg2-related arrhythmogenic right ventricular cardiomyopathy
Abstract
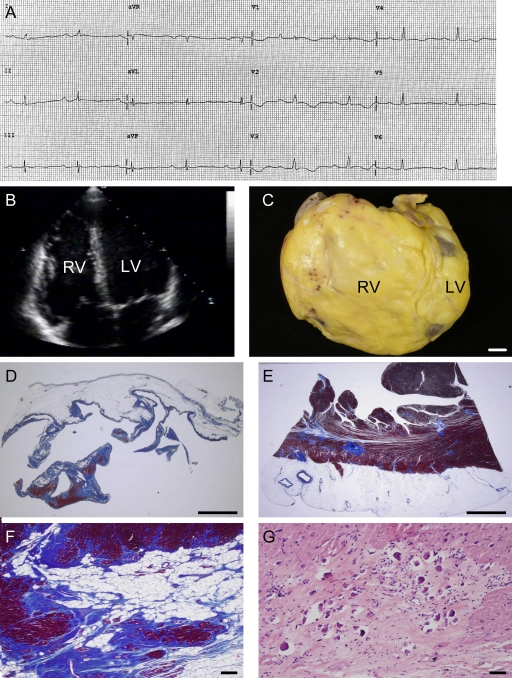
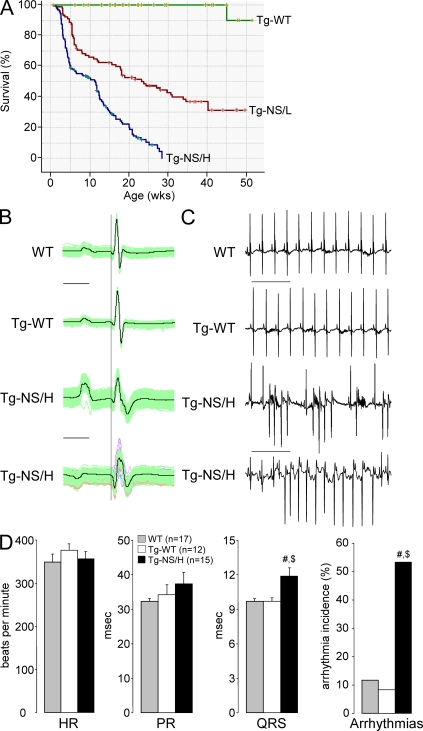
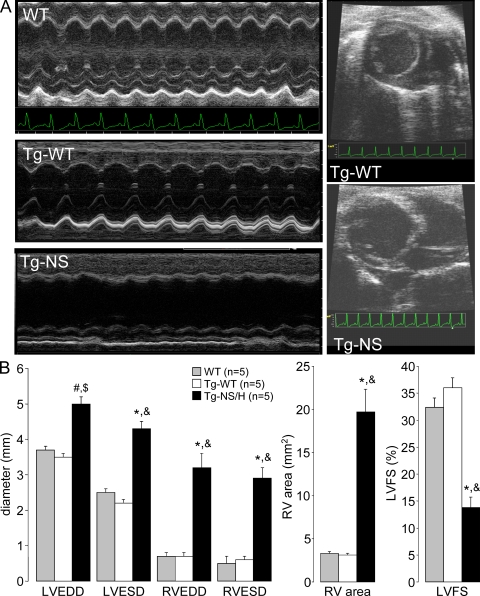
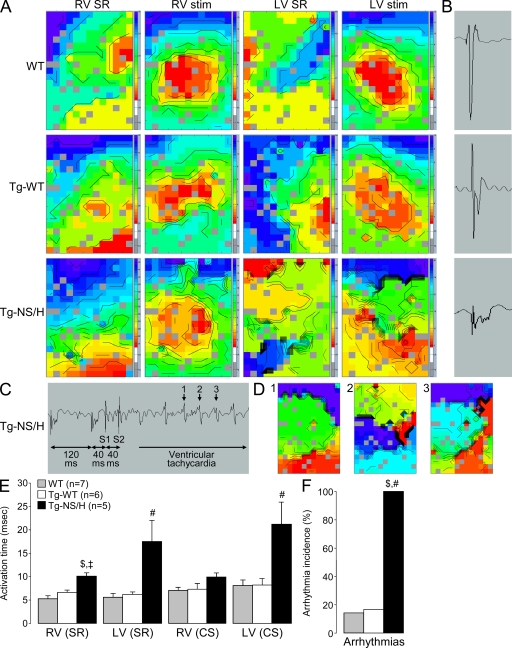
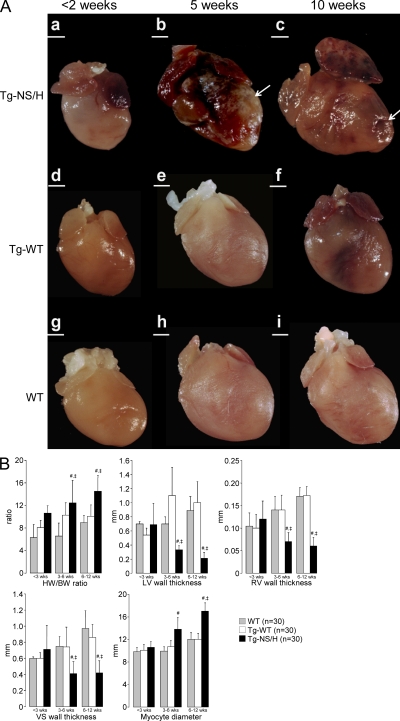
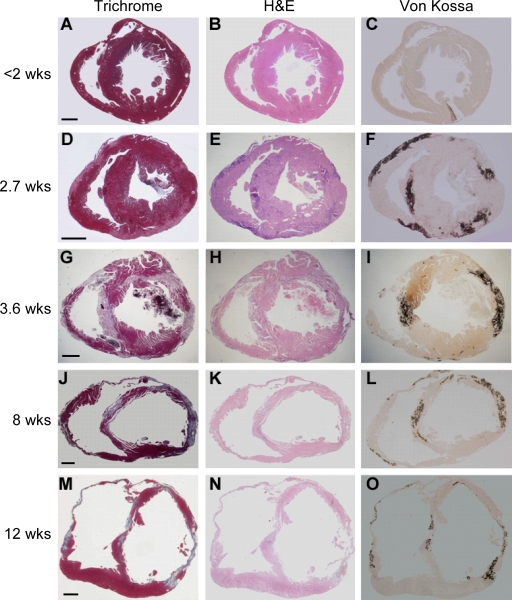
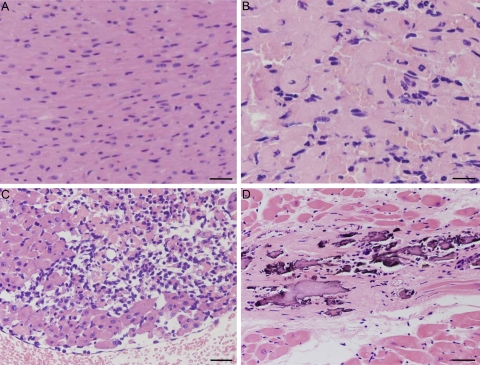
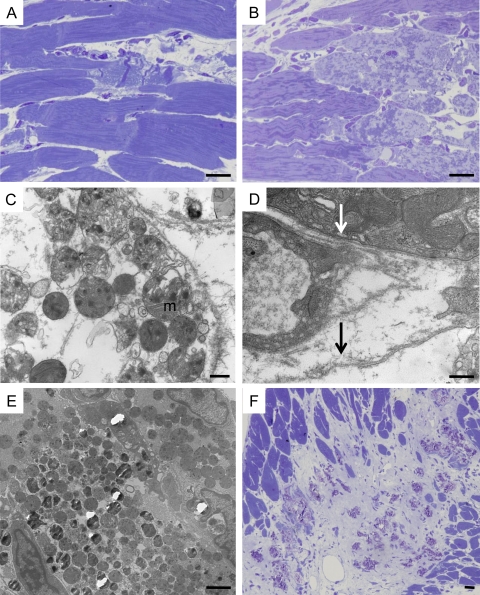
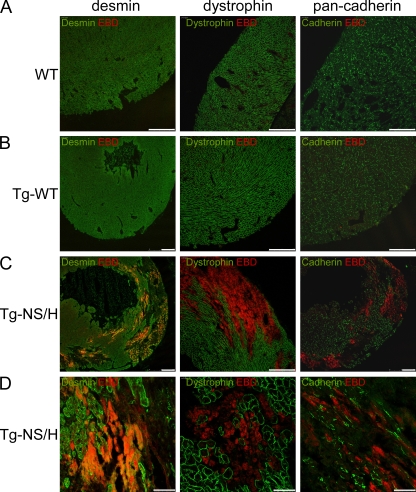
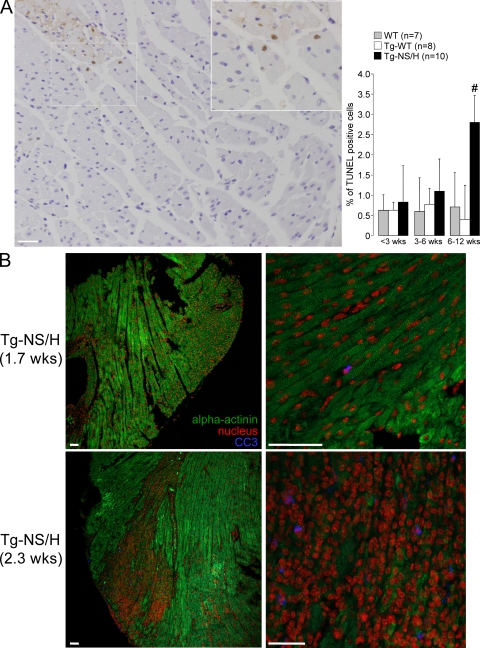
Mutations in the cardiac desmosomal protein desmoglein-2 (DSG2) are associated with arrhythmogenic right ventricular cardiomyopathy (ARVC). We studied the explanted heart of a proband carrying the DSG2-N266S mutation as well as transgenic mice (Tg-NS) with cardiac overexpression of the mouse equivalent of this mutation, N271S-dsg2, with the aim of investigating the pathophysiological mechanisms involved. Transgenic mice recapitulated the clinical features of ARVC, including sudden death at young age, spontaneous ventricular arrhythmias, cardiac dysfunction, and biventricular dilatation and aneurysms. Investigation of transgenic lines with different levels of transgene expression attested to a dose-dependent dominant-negative effect of the mutation. We demonstrate for the first time that myocyte necrosis is the key initiator of myocardial injury, triggering progressive myocardial damage, including an inflammatory response and massive calcification within the myocardium, followed by injury repair with fibrous tissue replacement, and myocardial atrophy. These observations were supported by findings in the explanted heart from the patient. Insight into mechanisms initiating myocardial damage in ARVC is a prerequisite to the future development of new therapies aimed at delaying onset or progression of the disease.
Figures
References
-
- Asimaki A., Syrris P., Wichter T., Matthias P., Saffitz J.E., McKenna W.J. 2007. A novel dominant mutation in plakoglobin causes arrhythmogenic right ventricular cardiomyopathy.Am. J. Hum. Genet. 81:964–973 - PMC - PubMed
-
- Bansal D., Miyake K., Vogel S.S., Groh S., Chen C.C., Williamson R., McNeil P.L., Campbell K.P. 2003. Defective membrane repair in dysferlin-deficient muscular dystrophy.Nature. 423:168–172 - PubMed
-
- Basso C., Thiene G., Corrado D., Angelini A., Nava A., Valente M. 1996. Arrhythmogenic right ventricular cardiomyopathy. Dysplasia, dystrophy, or myocarditis? Circulation. 94:983–991 - PubMed
-
- Basso C., Tsatsopoulou A., Thiene G., Anastasakis A., Valente M., Protonotarios N. 2001. “Petrified” right ventricle in long-standing naxos arrhythmogenic right ventricular cardiomyopathy.Circulation. 104:E132–E133 - PubMed
-
- Basso C., Czarnowska E., Della Barbera M., Bauce B., Beffagna G., Wlodarska E.K., Pilichou K., Ramondo A., Lorenzon A., Wozniek O., et al. 2006. Ultrastructural evidence of intercalated disc remodelling in arrhythmogenic right ventricular cardiomyopathy: an electron microscopy investigation on endomyocardial biopsies.Eur. Heart J. 27:1847–1854 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
