

Electrocardiographic features of arrhythmogenic right ventricular dysplasia
- PMID: 19635971
- PMCID: PMC2814546
- DOI: 10.1161/CIRCULATIONAHA.108.838821
Electrocardiographic features of arrhythmogenic right ventricular dysplasia
Abstract
Background: The purpose of this study was to reevaluate the ECG features of arrhythmogenic right ventricular dysplasia (ARVD). The second objective was to evaluate the sensitivity and specificity of the standard and newly proposed diagnostic ECG markers in the presence of a right bundle-branch block (RBBB).
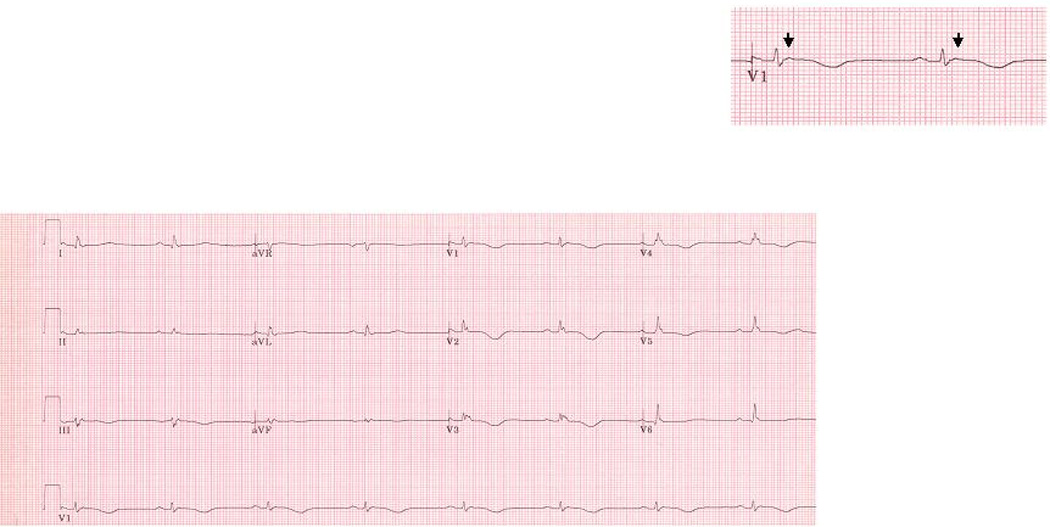
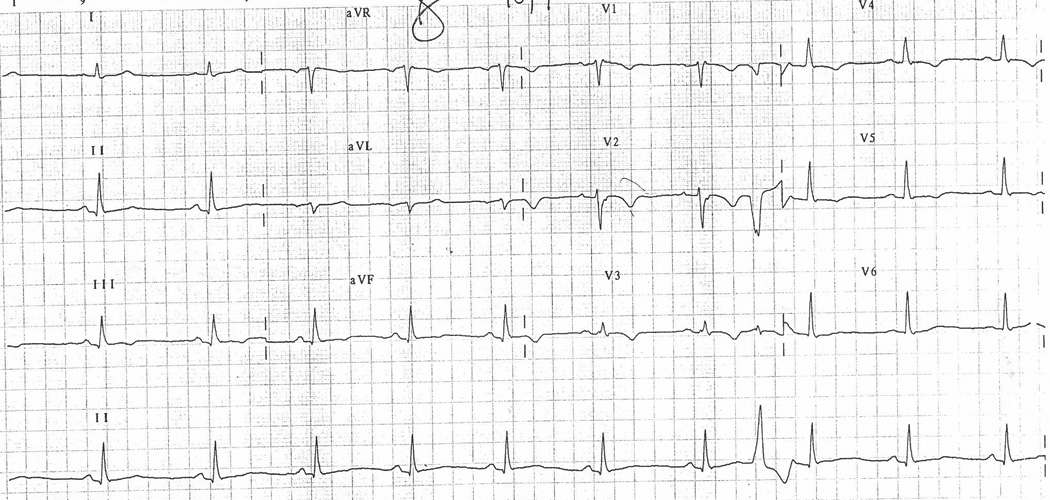
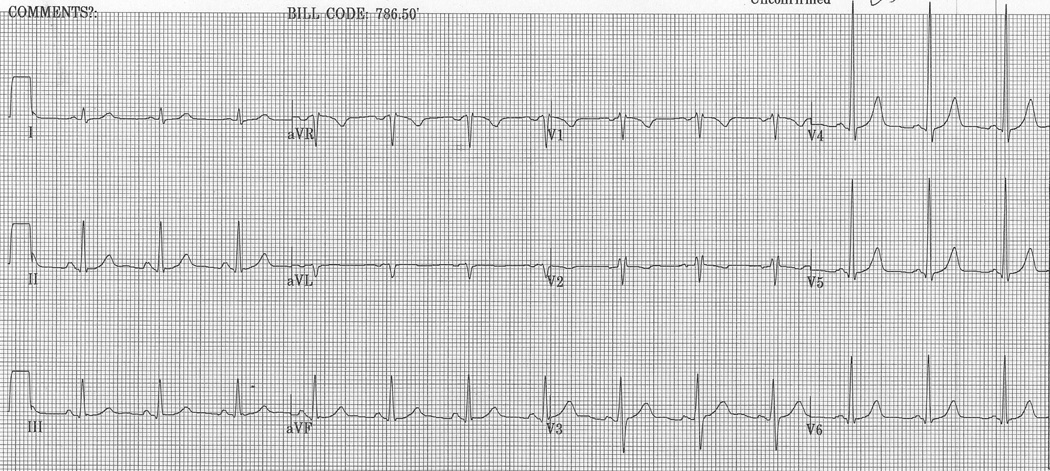
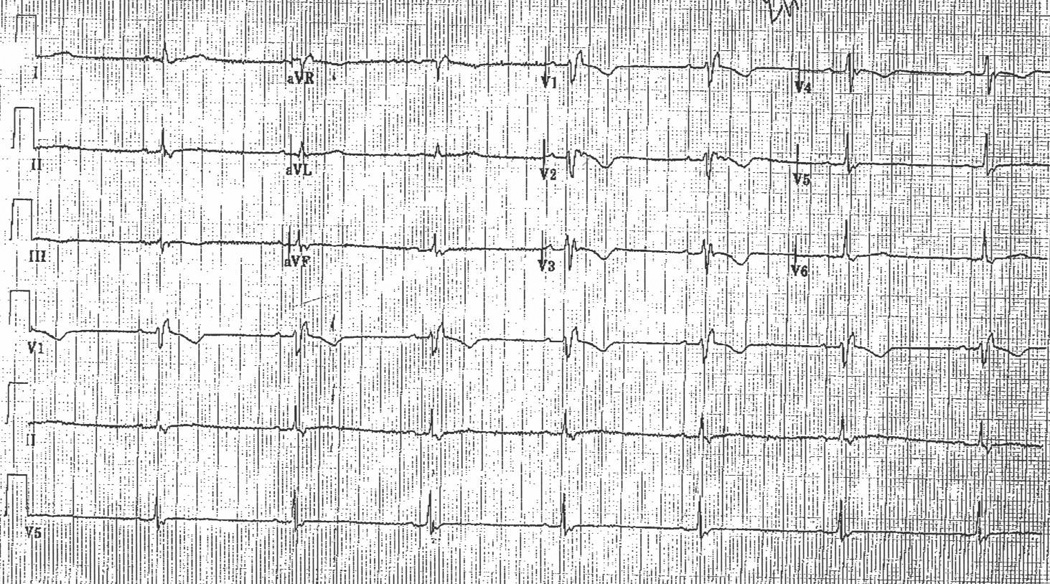
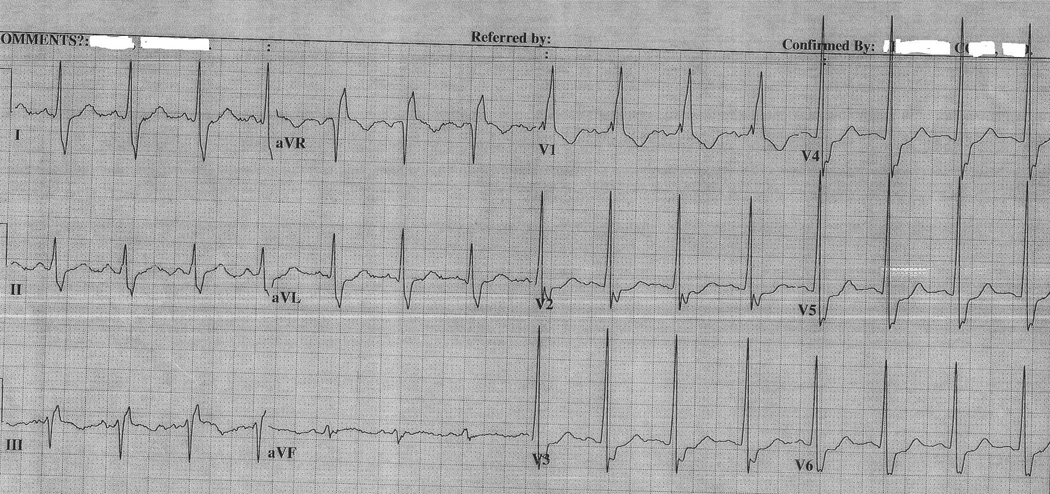
Methods and results: One hundred patients with ARVD (57 men; aged 39+/-15 years) and 57 controls (21 men; aged 40+/-17 years) were included. Among the 100 patients with ARVD, a complete RBBB was present in 17 patients, and 15 patients had an incomplete RBBB. T-wave inversion through V(3) demonstrated optimal sensitivity and specificity in both ARVD patients without a complete RBBB or incomplete RBBB (71% [95% confidence interval, 58% to 81%] and 96% [95% confidence interval, 81% to 100%], respectively) and in ARVD patients with incomplete RBBB (73% [95% confidence interval, 45% to 92%] and 95% [95% confidence interval, 77% to 100%], respectively). Between ARVD patients and controls with a complete RBBB, the only 2 parameters that differed were the prevalence of T-wave inversion through V(4) (59% versus 12%, respectively; P<0.05) and an r'/s ratio in V(1) <1 (88% versus 14%, respectively; P<0.005). In ARVD patients with complete RBBB, the most sensitive and specific parameter was an r'/s ratio <1.
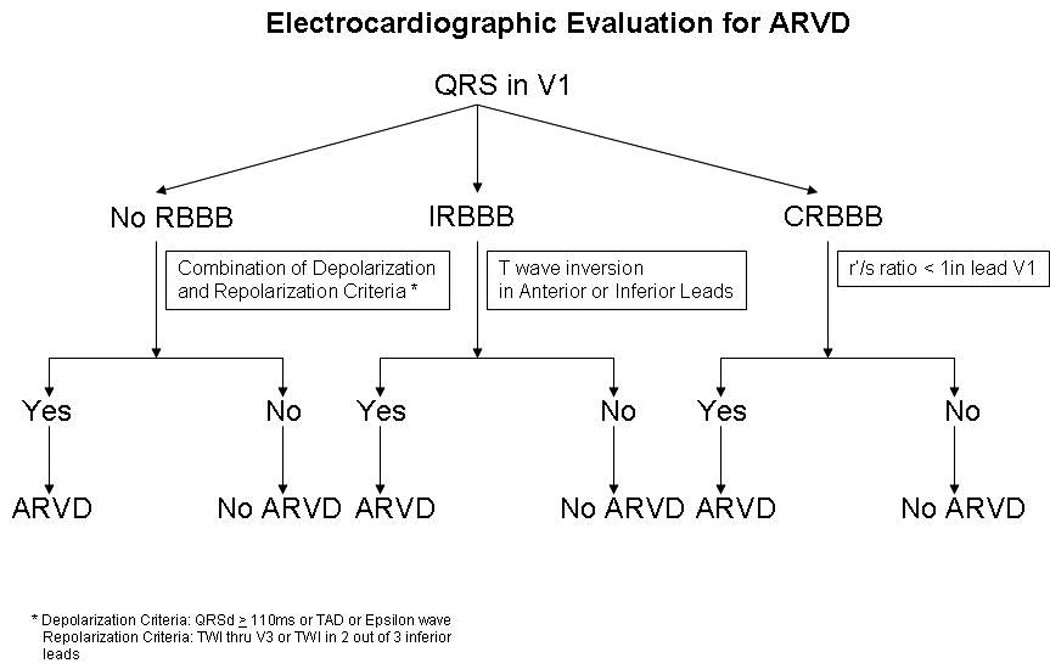
Conclusions: We evaluated comprehensively the diagnostic value of ECG markers for ARVD. On the basis of the findings, we propose an algorithm, with examination of QRS morphology being the first step, for ECG evaluation of ARVD patients. Definite criteria are then applied on the basis of the presence of no RBBB, incomplete RBBB, and complete RBBB to obtain the best diagnostic utility of the ECG.
Figures
Comment in
-
Letter by Thomas et al regarding article, "Electrocardiographic features of arrhythmogenic right ventricular dysplasia".Circulation. 2010 May 18;121(19):e404; author reply e406. doi: 10.1161/CIRCULATIONAHA.109.901876. Circulation. 2010. PMID: 20479160 No abstract available.
-
Letter by Assenza et al regarding article, "Electrocardiographic features of arrhythmogenic right ventricular dysplasia".Circulation. 2010 May 18;121(19):e405; author reply e406. doi: 10.1161/CIRCULATIONAHA.109.908889. Circulation. 2010. PMID: 20479161 No abstract available.
References
-
- Marcus FI, Fontaine GH, Guiraudon G, Frank R, Laurenceau JL, Malergue C, Grosgogeat Y. Right ventricular dysplasia: a report of 24 adult cases. Circulation. 1982;65:384–398. - PubMed
-
- Dalal D, Nasir K, Bomma C, Prakasa K, Tandri H, Piccini J, Roguin A, Tichnell C, James C, Russell SD, Judge DP, Abraham T, Spevak PJ, Bluemke DA, Calkins H. Arrhythmogenic right ventricular dysplasia: a United States experience. Circulation. 2005;112:3823–3832. - PubMed
-
- Corrado D, Basso C, Thiene G, McKenna WJ, Davies MJ, Fontaliran F, Nava A, Silvestri F, Blomstrom-Lundqvist C, Wlodarska EK, Fontaine G, Camerini F. Spectrum of clinicopathologic manifestations of arrhythmogenic right ventricular cardiomyopathy/dysplasia: a multicenter study. J Am Coll Cardiol. 1997;30:1512–1520. - PubMed
-
- Basso C, Thiene G, Corrado D, Angelini A, Nava A, Valente M. Arrhythmogenic right ventricular cardiomyopathy. Dysplasia, dystrophy, or myocarditis? Circulation. 1996;94:983–991. - PubMed
-
- Gerull B, Heuser A, Wichter T, Paul M, Basson CT, McDermott DA, Lerman BB, Markowitz SM, Ellinor PT, MacRae CA, Peters S, Grossmann KS, Michely B, Sasse-Klaassen S, Birchmeier W, Dietz R, Breithardt G, Schulze-Bahr E, Thierfelder L. Mutations in the desmosomal protein plakophilin-2 are common in arrhythmogenic right ventricular cardiomyopathy. Nat Genet. 2004;36:1162–1164. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
