

Prostate cancer-specific mortality after radical prostatectomy for patients treated in the prostate-specific antigen era
- PMID: 19636023
- PMCID: PMC3651598
- DOI: 10.1200/JCO.2008.18.2501
Prostate cancer-specific mortality after radical prostatectomy for patients treated in the prostate-specific antigen era
Abstract
Purpose: The long-term risk of prostate cancer-specific mortality (PCSM) after radical prostatectomy is poorly defined for patients treated in the era of widespread prostate-specific antigen (PSA) screening. Models that predict the risk of PCSM are needed for patient counseling and clinical trial design.
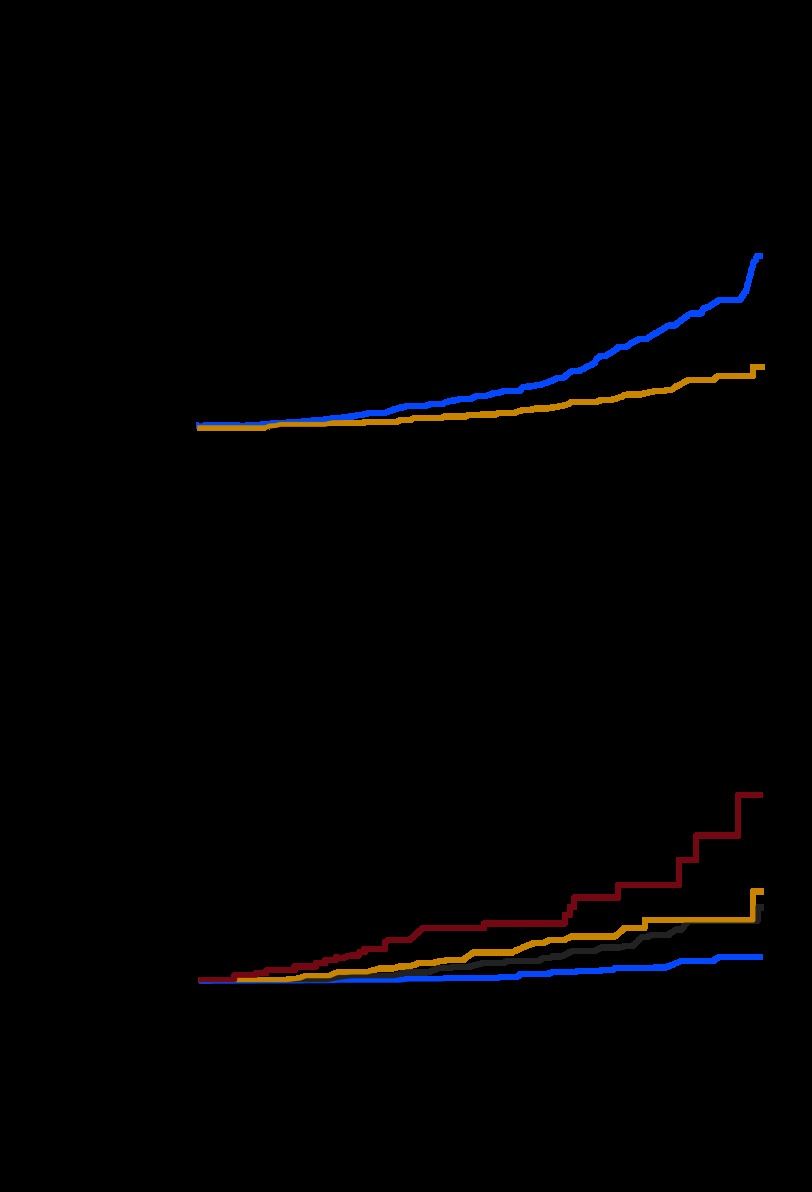
Methods: A multi-institutional cohort of 12,677 patients treated with radical prostatectomy between 1987 and 2005 was analyzed for the risk of PCSM. Patient clinical information and treatment outcome was modeled using Fine and Gray competing risk regression analysis to predict PCSM.
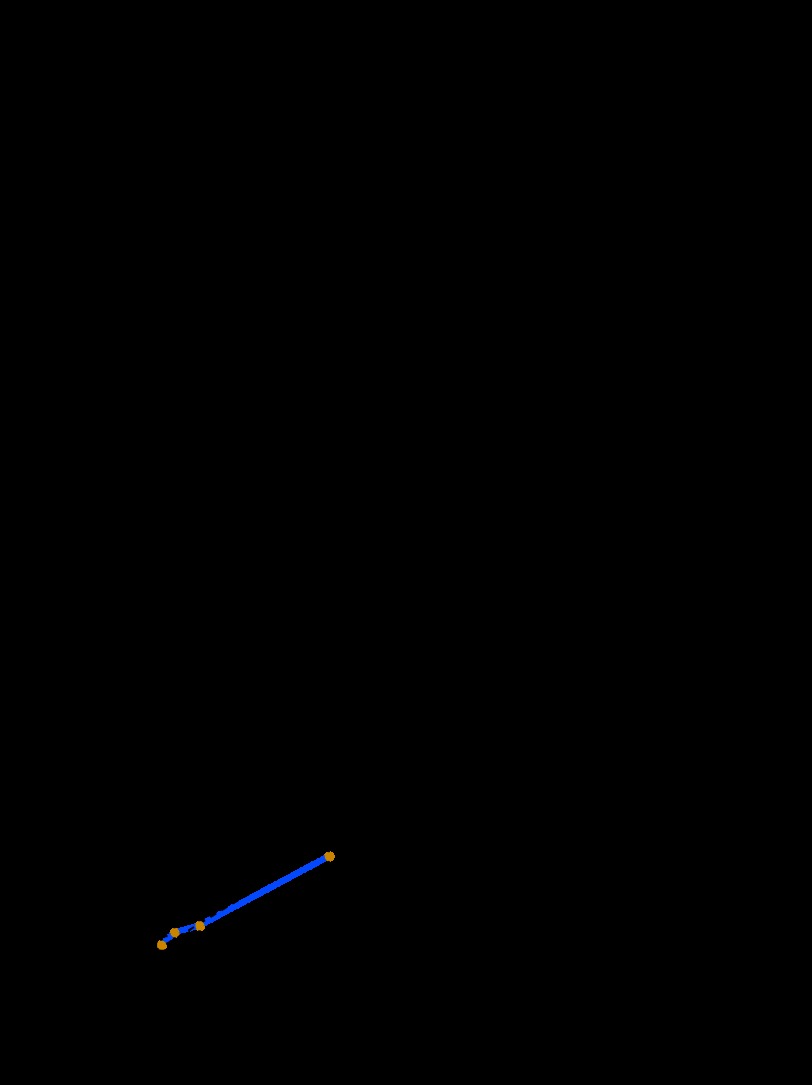
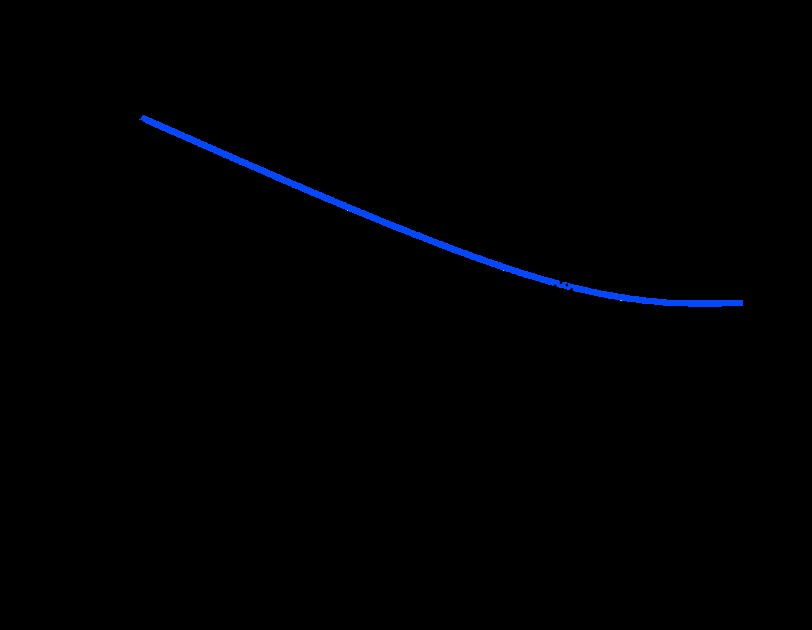
Results: Fifteen-year PCSM and all-cause mortality were 12% and 38%, respectively. The estimated PCSM ranged from 5% to 38% for patients in the lowest and highest quartiles of predicted risk of PSA-defined recurrence, based on a popular nomogram. Biopsy Gleason grade, PSA, and year of surgery were associated with PCSM. A nomogram predicting the 15-year risk of PCSM was developed, and the externally validated concordance index was 0.82. Neither preoperative PSA velocity nor body mass index improved the model's accuracy. Only 4% of contemporary patients had a predicted 15-year PCSM of greater than 5%.
Conclusion: Few patients will die from prostate cancer within 15 years of radical prostatectomy, despite the presence of adverse clinical features. This favorable prognosis may be related to the effectiveness of radical prostatectomy (with or without secondary therapy) or the low lethality of screen-detected cancers. Given the limited ability to identify contemporary patients at substantially elevated risk of PCSM on the basis of clinical features alone, the need for novel markers specifically associated with the biology of lethal prostate cancer is evident.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Words of wisdom. Re: Prostate cancer-specific mortality after radical prostatectomy for patients treated in the prostate-specific antigen era.Eur Urol. 2009 Dec;56(6):1089-90. doi: 10.1016/j.eururo.2009.09.011. Eur Urol. 2009. PMID: 20965041 No abstract available.
References
-
- Albertsen PC, Hanley JA, Fine J. 20-year outcomes following conservative management of clinically localized prostate cancer. JAMA. 2005;293:2095–2101. - PubMed
-
- Johansson JE, Andren O, Andersson SO, et al. Natural history of early, localized prostate cancer. JAMA. 2004;291:2713–2719. - PubMed
-
- Bill-Axelson A, Holmberg L, Ruutu M, et al. Radical prostatectomy versus watchful waiting in early prostate cancer. N Engl J Med. 2005;352:1977–1984. - PubMed
-
- Draisma G, Boer R, Otto SJ, et al. Lead times and overdetection due to prostate-specific antigen screening: Estimates from the European Randomized Study of Screening for Prostate Cancer. J Natl Cancer Inst. 2003;95:868–878. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
