

Systematic review of the relation between smokeless tobacco and cancer in Europe and North America
- PMID: 19638245
- PMCID: PMC2744672
- DOI: 10.1186/1741-7015-7-36
Systematic review of the relation between smokeless tobacco and cancer in Europe and North America
Abstract
Background: Interest is rising in smokeless tobacco as a safer alternative to smoking, but published reviews on smokeless tobacco and cancer are limited. We review North American and European studies and compare effects of smokeless tobacco and smoking.
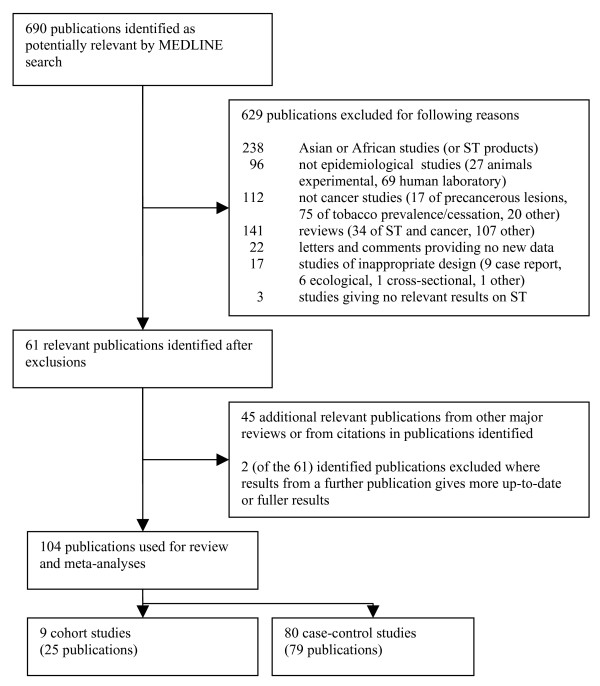
Methods: We obtained papers from MEDLINE searches, published reviews and secondary references describing epidemiological cohort and case-control studies relating any form of cancer to smokeless tobacco use. For each study, details were abstracted on design, smokeless tobacco exposure, cancers studied, analysis methods and adjustment for smoking and other factors. For each cancer, relative risks or odds ratios with 95% confidence intervals were tabulated. Overall, and also for USA and Scandinavia separately, meta-analyses were conducted using all available estimates, smoking-adjusted estimates, or estimates for never smokers. For seven cancers, smoking-attributable deaths in US men in 2005 were compared with deaths attributable to introducing smokeless tobacco into a population of never-smoking men.
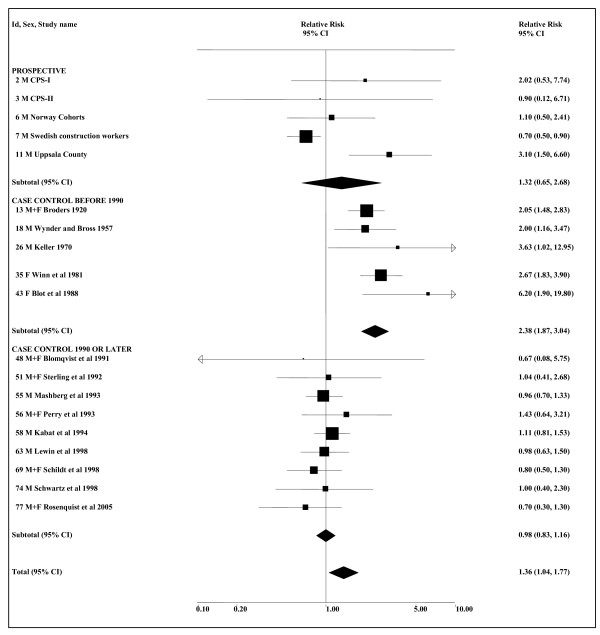
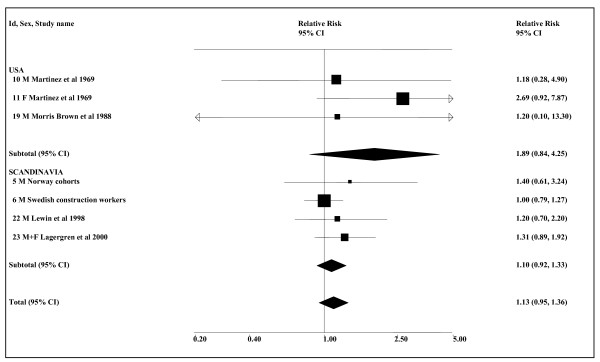
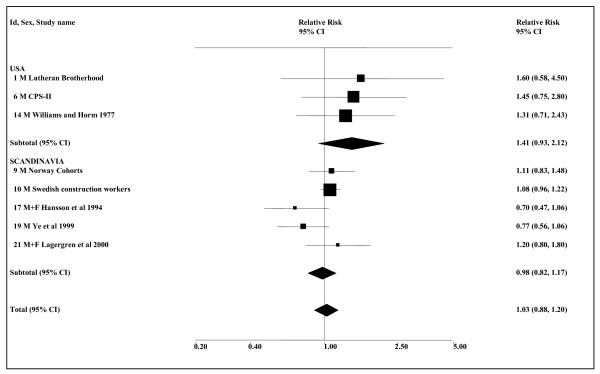
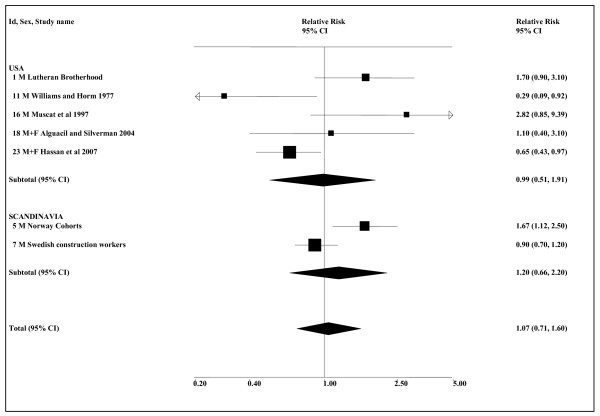
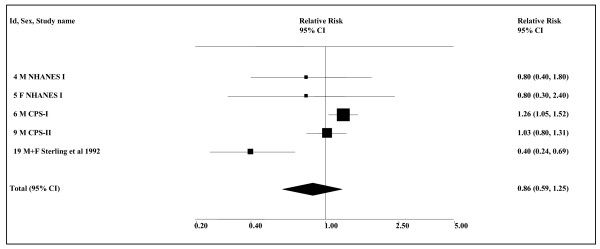
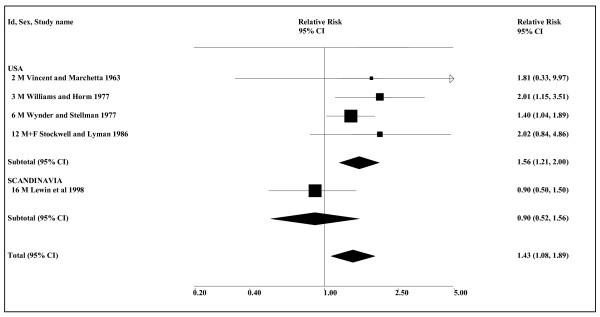
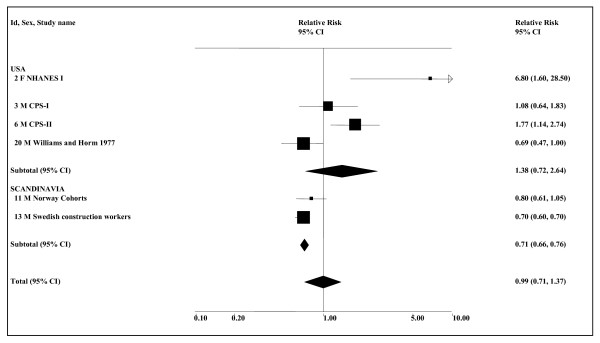
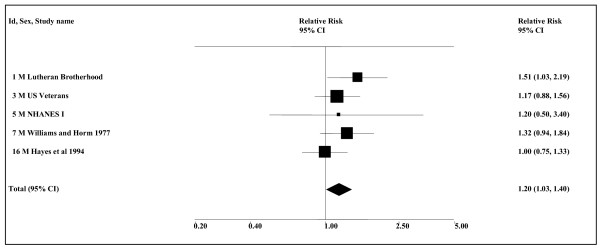
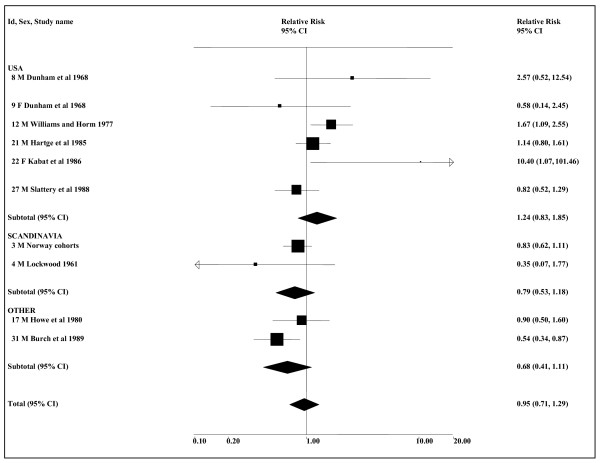
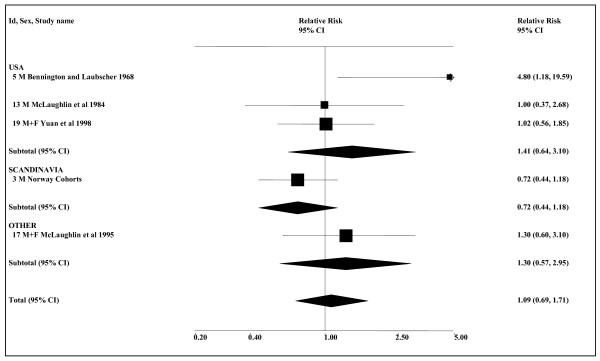
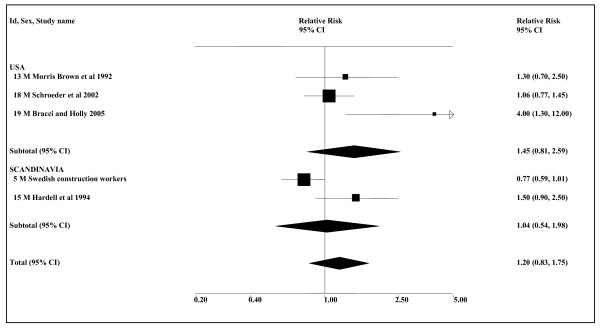
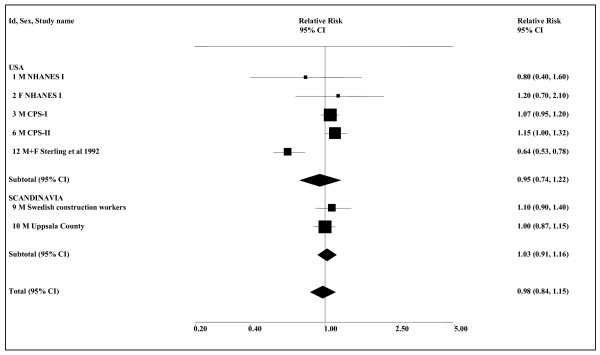
Results: Eighty-nine studies were identified; 62 US and 18 Scandinavian. Forty-six (52%) controlled for smoking. Random-effects meta-analysis estimates for most sites showed little association. Smoking-adjusted estimates were only significant for oropharyngeal cancer (1.36, CI 1.04-1.77, n = 19) and prostate cancer (1.29, 1.07-1.55, n = 4). The oropharyngeal association disappeared for estimates published since 1990 (1.00, 0.83-1.20, n = 14), for Scandinavia (0.97, 0.68-1.37, n = 7), and for alcohol-adjusted estimates (1.07, 0.84-1.37, n = 10). Any effect of current US products or Scandinavian snuff seems very limited. The prostate cancer data are inadequate for a clear conclusion.Some meta-analyses suggest a possible effect for oesophagus, pancreas, larynx and kidney cancer, but other cancers show no effect of smokeless tobacco. Any possible effects are not evident in Scandinavia. Of 142,205 smoking-related male US cancer deaths in 2005, 104,737 are smoking-attributable. Smokeless tobacco-attributable deaths would be 1,102 (1.1%) if as many used smokeless tobacco as had smoked, and 2,081 (2.0%) if everyone used smokeless tobacco.
Conclusion: An increased risk of oropharyngeal cancer is evident most clearly for past smokeless tobacco use in the USA, but not for Scandinavian snuff. Effects of smokeless tobacco use on other cancers are not clearly demonstrated. Risk from modern products is much less than for smoking.
Figures
Comment in
-
Review of epidemiologic data on the debate over smokeless tobacco's role in harm reduction.BMC Med. 2009 Oct 19;7:61. doi: 10.1186/1741-7015-7-61. BMC Med. 2009. PMID: 19840371 Free PMC article. Review.
References
-
- International Agency for Research on Cancer. Smokeless tobacco and some tobacco-specific N-nitrosamines. [IARC Monographs on the evaluation of carcinogenic risks to humans.] Vol. 89. Lyon, France: IARC; 2007. http://monographs.iarc.fr/index.php - PMC - PubMed
-
- Scientific Committee on Emerging and Newly Identified Health Risks (SCENIHR) Health effects of smokeless tobacco products. Brussels: European Commission, Health & Consumer Protection Directorate-General; 2008. http://ec.europa.eu/health/ph_risk/committees/04_scenihr/docs/scenihr_o_...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
