

Starving the addiction: new opportunities for durable suppression of AR signaling in prostate cancer
- PMID: 19638458
- PMCID: PMC2842118
- DOI: 10.1158/1078-0432.CCR-08-2660
Starving the addiction: new opportunities for durable suppression of AR signaling in prostate cancer
Abstract
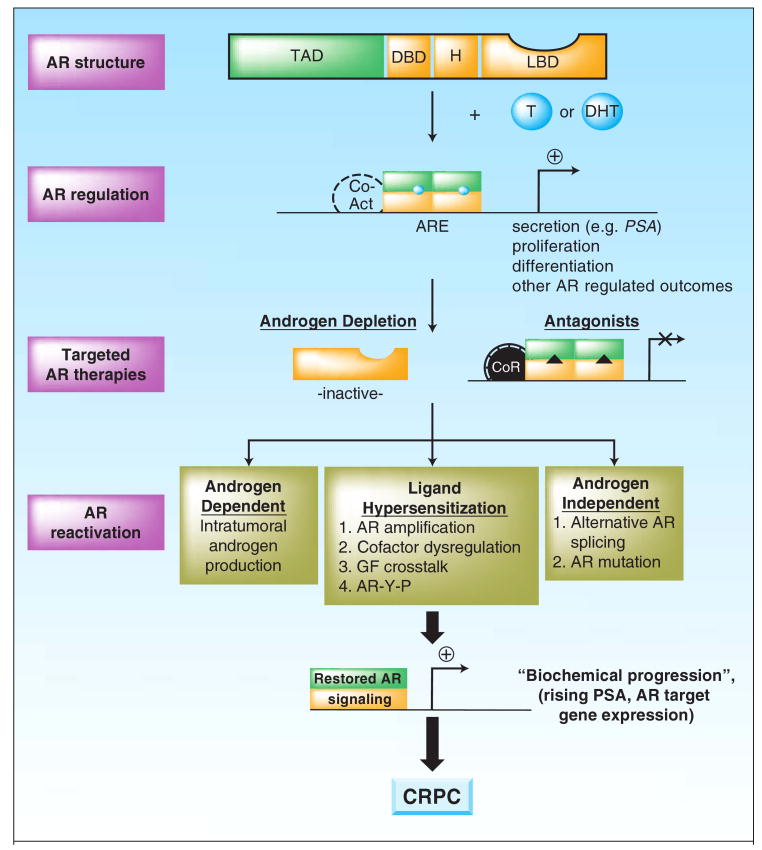
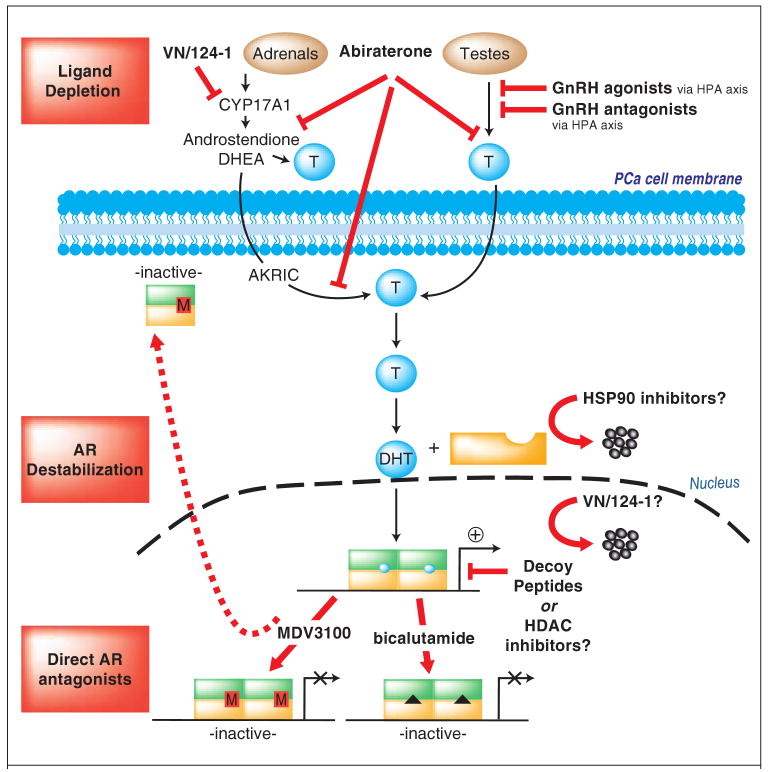
Clinical data and models of human disease indicate that androgen receptor (AR) activity is essential for prostate cancer development, growth, and progression. The dependence of prostatic adenocarcinoma on AR signaling at all stages of disease has thereby been exploited in the treatment of disseminated tumors, for which ablation of AR function is the goal of first-line therapy. Although these strategies are initially effective, recurrent tumors arise with restored AR activity, and no durable treatment has yet been identified to combat this stage of disease. New insights into AR regulation and the mechanisms underlying resurgent AR activity have provided fertile ground for the development of novel strategies to more effectively inhibit receptor activity and prolong the transition to therapeutic failure.
Figures
References
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007;57:43–66. - PubMed
-
- Klein EA, Ciezki J, Kupelian PA, Mahadevan A. Outcomes for intermediate risk prostate cancer: Are there advantages for surgery, external radiation, or brachytherapy? Urol Oncol. 2009;27:67–71. - PubMed
-
- Loblaw DA, Virgo KS, Nam R, et al. Initial hormonal management of androgen-sensitive metastatic, recurrent, or progressive prostate cancer: 2006 update of an American Society of Clinical Oncology practice guideline. J Clin Oncol. 2007;25:1596–605. - PubMed
-
- Taplin ME. Drug insight: role of the androgen receptor in the development and progression of prostate cancer. Nat Clin Pract Oncol. 2007;4:236–44. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
