

Cytological surveillance compared with immediate referral for colposcopy in management of women with low grade cervical abnormalities: multicentre randomised controlled trial
- PMID: 19638646
- PMCID: PMC2718083
- DOI: 10.1136/bmj.b2546
Cytological surveillance compared with immediate referral for colposcopy in management of women with low grade cervical abnormalities: multicentre randomised controlled trial
Abstract
Objectives: To examine the effectiveness of cytological surveillance in primary care compared with immediate referral for colposcopic examination in women with low grade abnormal results on cervical cytology tests.
Design: Multicentre individually randomised controlled trial.
Setting: NHS cervical screening programmes in Grampian, Tayside, and Nottingham.
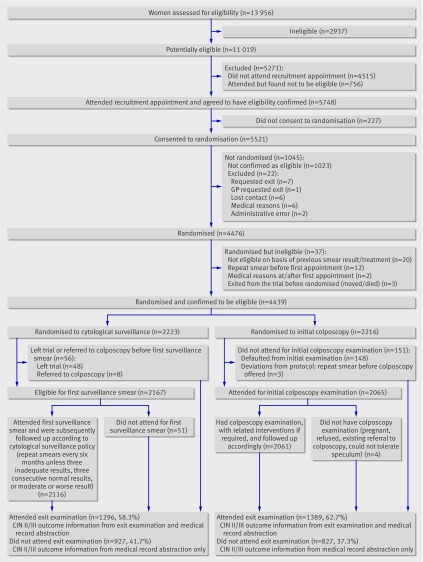
Participants: 4439 women, aged 20-59, with a cytology result showing borderline nuclear abnormalities or mild dyskaryosis, October 1999-October 2002.
Interventions: Cytological screening every six months in primary care (n=2223) or referral for colposcopy and related interventions (n=2216). All women were followed for three years, concluding with an exit appointment at which colposcopic examination was undertaken. Colposcopists assessing outcome at this appointment were blinded to randomisation.
Main outcome measures: Primary end point: cumulative incidence of cervical intraepithelial neoplasia grade II or more severe disease. Other end points: cervical intraepithelial neoplasia grade III or worse, clinically significant anxiety and depression, other self reported after effects, and rates of non-attendance. Analysis was by intention to treat; all those randomised were included.
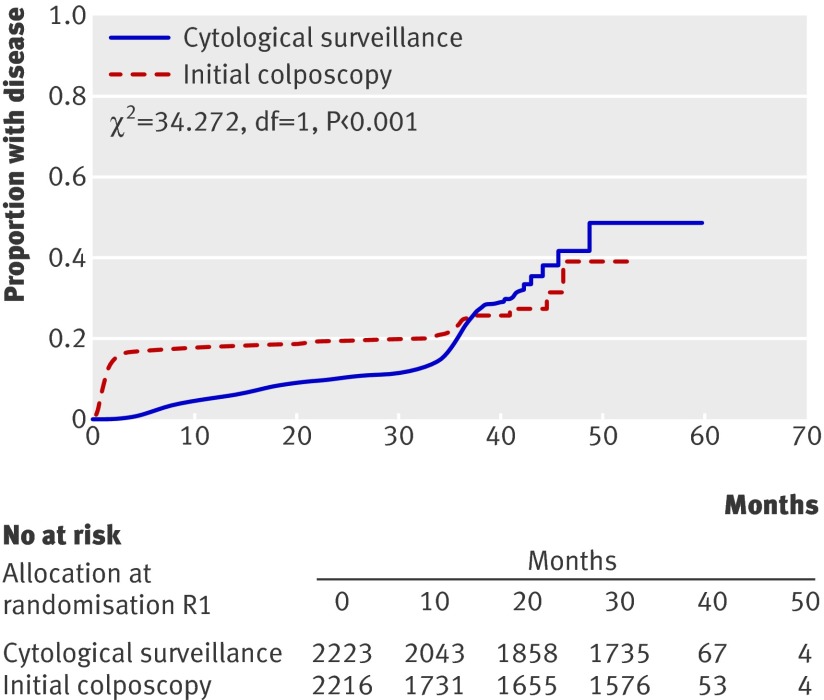
Results: The cumulative incidence of cervical intraepithelial neoplasia grade II or worse was 79 per 1000 person years in the colposcopy arm and 58 per 1000 person years in the cytological surveillance arm (relative risk 1.37, 95% confidence interval 1.19 to 1.57). This difference was less marked for cervical intraepithelial neoplasia grade III or more severe disease, but the incidence was still higher in the colposcopy arm (relative risk 1.26, 1.04 to 1.53). Among women randomised to immediate colposcopy, 79% (74.9% to 82.5%) of cases of cervical intraepithelial neoplasia grade II or worse were diagnosed at the time of the immediate colposcopy, while among women randomised to cytological surveillance, 77% (72.1% to 81.2%) of cases were detected by surveillance cytology and related interventions. Similar proportions of women were anxious or depressed in the two arms. A higher proportion of women in the colposcopy arm reported after effects, and these were of longer duration and more severe. Non-attendance was low in both arms.
Conclusion: The more marked difference between the arms in the occurrence of cervical intraepithelial neoplasia grade II or worse than in the occurrence of grade III or worse can probably be accounted for by the spontaneous regression of some cases of grade II neoplasia. Compared with cytological surveillance, a policy of immediate colposcopy detects more cervical intraepithelial neoplasia grade II or worse, and some more grade III or worse, but might lead to overtreatment. Such a policy is associated with a higher rate of reported after effects, which are more severe and of longer duration than those associated with cytological surveillance.
Trial registration: ISRCTN 34841617.
Conflict of interest statement
Competing interests: During the past five years ID has served on British and European Boards advising GlaxoSmithKline regarding the connection between human papillomavirus and cervical neoplasia, for which he has received expenses and fees for professional services. He has participated in a symposium sponsored by GlaxoSmithKline as part of a EUROGIN conference in Paris and was partly sponsored as a result. He has assisted in GlaxoSmithKline’s and MSD Sanofi Pasteur’s education programmes increasing professional awareness of the link between the human papillomavirus and cervical neoplasia, receiving fees for his professional services in creating a set of educational slides and lecturing to doctors and nurses. JL has received fees from GlaxoSmithKline as a member of an independent data and safety monitoring committee for a trial of the efficacy of vaccination against HSV. NG was reimbursed for attending an international clinical advisory board on health related quality of life issues related to cervical cancer in April 2005 by GlaxoSmithKline. From 2003 until September 2007 DJ was director of clinical research into papillomavirus vaccines for GlaxoSmithKline Biologicals and continues to act as a consultant to GSK.
Figures
Comment in
-
Managing low grade and borderline cervical abnormalities.BMJ. 2009 Jul 28;339:b3014. doi: 10.1136/bmj.b3014. BMJ. 2009. PMID: 19638653 No abstract available.
-
Immediate colposcopy referral in women with low-grade abnormal results on cervical cytology detects more CIN2 or worse lesions than cytological surveillance in primary care, but might lead to overtreatment.Evid Based Med. 2010 Feb;15(1):13-4. doi: 10.1136/ebm.15.1.13. Evid Based Med. 2010. PMID: 20176871 No abstract available.
References
-
- Vizcaino AP, Moreno V, Bosch FX, Munoz N, Barros- Dios XM, Borras J, et al. International trends in incidence of cervical cancer: II. Squamous-cell carcinoma. Int J Cancer 2000;86:429-35. - PubMed
-
- Peto J, Gilham C, Fletcher O, Matthews FE. The cervical cancer epidemic that screening has prevented in the UK. Lancet 2004;364:249-56. - PubMed
-
- Liu S, Semenciw R, Probert A, Mao Y. Cervical cancer in Canada: changing patterns in incidence and mortality. Int J Gynecol Cancer 2001;11:24-31. - PubMed
-
- Bray F, Loos AH, McCarron P, Weiderpass E, Arbyn M, Moller H, et al. Trends in cervical squamous cell carcinoma incidence in 13 European countries: changing risk and the effects of screening. Cancer Epidemiol Biomarkers Prev 2005;14:677-86. - PubMed