

APACHE III outcome prediction in patients admitted to the intensive care unit after liver transplantation: a retrospective cohort study
- PMID: 19640303
- PMCID: PMC2726122
- DOI: 10.1186/1471-2482-9-11
APACHE III outcome prediction in patients admitted to the intensive care unit after liver transplantation: a retrospective cohort study
Abstract
Background: The Acute Physiology and Chronic Health Evaluation (APACHE) III prognostic system has not been previously validated in patients admitted to the intensive care unit (ICU) after orthotopic liver transplantation (OLT). We hypothesized that APACHE III would perform satisfactorily in patients after OLT METHODS: A retrospective cohort study was performed. Patients admitted to the ICU after OLT between July 1996 and May 2008 were identified. Data were abstracted from the institutional APACHE III and liver transplantation databases and individual patient medical records. Standardized mortality ratios (with 95% confidence intervals) were calculated by dividing the observed mortality rates by the rates predicted by APACHE III. The area under the receiver operating characteristic curve (AUC) and the Hosmer-Lemeshow C statistic were used to assess, respectively, discrimination and calibration of APACHE III.
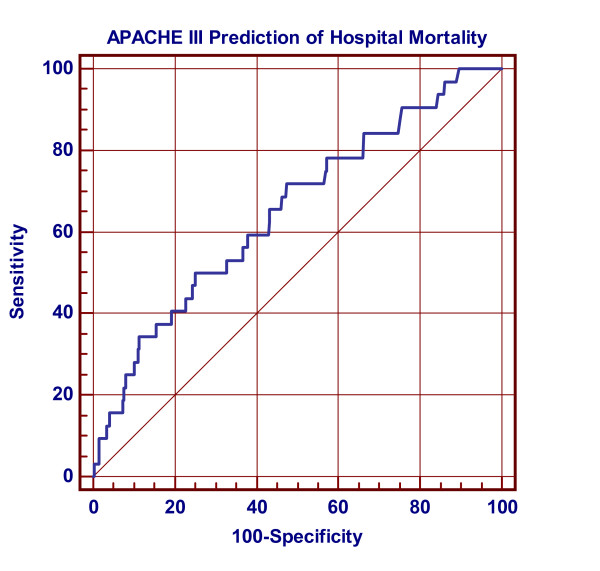
Results: APACHE III data were available for 918 admissions after OLT. Mean (standard deviation [SD]) APACHE III (APIII) and Acute Physiology (APS) scores on the day of transplant were 60.5 (25.8) and 50.8 (23.6), respectively. Mean (SD) predicted ICU and hospital mortality rates were 7.3% (15.4) and 10.6% (18.9), respectively. The observed ICU and hospital mortality rates were 1.1% and 3.4%, respectively. The standardized ICU and hospital mortality ratios with their 95% C.I. were 0.15 (0.07 to 0.27) and 0.32 (0.22 to 0.45), respectively. There were statistically significant differences in APS, APIII, predicted ICU and predicted hospital mortality between survivors and non-survivors. In predicting mortality, the AUC of APACHE III prediction of hospital death was 0.65 (95% CI, 0.62 to 0.68). The Hosmer-Lemeshow C statistic was 5.288 with a p value of 0.871 (10 degrees of freedom).
Conclusion: APACHE III discriminates poorly between survivors and non-survivors of patients admitted to the ICU after OLT. Though APACHE III has been shown to be valid in heterogenous populations and in certain groups of patients with specific diagnoses, it should be used with caution - if used at all - in recipients of liver transplantation.
Figures
Similar articles
-
The acute physiology and chronic health evaluation III outcome prediction in patients admitted to the intensive care unit after pneumonectomy.J Cardiothorac Vasc Anesth. 2007 Dec;21(6):832-7. doi: 10.1053/j.jvca.2006.12.005. Epub 2007 Mar 6. J Cardiothorac Vasc Anesth. 2007. PMID: 18068061
-
Acute Physiology and Chronic Health Evaluation (APACHE) III outcome prediction after major vascular surgery.J Cardiothorac Vasc Anesth. 2008 Oct;22(5):713-8. doi: 10.1053/j.jvca.2008.01.009. Epub 2008 Mar 28. J Cardiothorac Vasc Anesth. 2008. PMID: 18922428
-
Intensive care unit support and Acute Physiology and Chronic Health Evaluation III performance in hematopoietic stem cell transplant recipients.Crit Care Med. 2003 Jun;31(6):1715-21. doi: 10.1097/01.CCM.0000065761.51367.2D. Crit Care Med. 2003. PMID: 12794410
-
Nursing Team Workload and the Apache Index of Gravity of Patients Post Liver Transplantation: A Cohort Study.Transplant Proc. 2022 Oct;54(8):2295-2300. doi: 10.1016/j.transproceed.2022.08.039. Epub 2022 Oct 11. Transplant Proc. 2022. PMID: 36229278 Review.
-
APACHE scoring system and pressure injury risk for intensive care patients: A systematic review and meta-analysis.Wound Repair Regen. 2022 Jul;30(4):498-508. doi: 10.1111/wrr.13021. Epub 2022 Jun 22. Wound Repair Regen. 2022. PMID: 35589532
Cited by
-
APACHE III Outcome Prediction in Patients Admitted to the Intensive Care Unit with Sepsis Associated Acute Lung Injury.PLoS One. 2015 Sep 30;10(9):e0139374. doi: 10.1371/journal.pone.0139374. eCollection 2015. PLoS One. 2015. PMID: 26422633 Free PMC article. Clinical Trial.
-
[Validation of APACHE IV score in postoperative liver transplantation in southern Brazil: a cohort study].Braz J Anesthesiol. 2019 May-Jun;69(3):279-283. doi: 10.1016/j.bjan.2018.11.010. Epub 2019 May 7. Braz J Anesthesiol. 2019. PMID: 31072607 Free PMC article.
-
Predicting outcomes in patients with sepsis-associated encephalopathy using prefrontal functional connectivity analysis.Sci Rep. 2025 May 23;15(1):18040. doi: 10.1038/s41598-025-02658-9. Sci Rep. 2025. PMID: 40410353 Free PMC article.
-
Predictors of the outcomes of acute-on-chronic hepatitis B liver failure.World J Gastroenterol. 2012 Sep 28;18(36):5078-83. doi: 10.3748/wjg.v18.i36.5078. World J Gastroenterol. 2012. PMID: 23049217 Free PMC article.
-
Predictive factors of short term outcome after liver transplantation: A review.World J Gastroenterol. 2016 Jul 14;22(26):5936-49. doi: 10.3748/wjg.v22.i26.5936. World J Gastroenterol. 2016. PMID: 27468188 Free PMC article. Review.
References
-
- Moreno RP, Metnitz PG, Almeida E, Jordan B, Bauer P, Campos RA, Iapichino G, Edbrooke D, Capuzzo M, Le Gall JR, et al. SAPS 3 – From evaluation of the patient to evaluation of the intensive care unit. Part 2: Development of a prognostic model for hospital mortality at ICU admission. Intensive Care Med. 2005;31:1345–1355. doi: 10.1007/s00134-005-2763-5. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
