

Is atherectomy the best first-line therapy for limb salvage in patients with critical limb ischemia?
- PMID: 19640919
- PMCID: PMC2897235
- DOI: 10.1177/1538574409334825
Is atherectomy the best first-line therapy for limb salvage in patients with critical limb ischemia?
Abstract
Objective: To determine the efficacy of atherectomy for limb salvage compared with open bypass in patients with critical limb ischemia.
Methods: Ninety-nine consecutive bypass and atherectomy procedures performed for critical limb ischemia between January 2003 and October 2006 were reviewed.
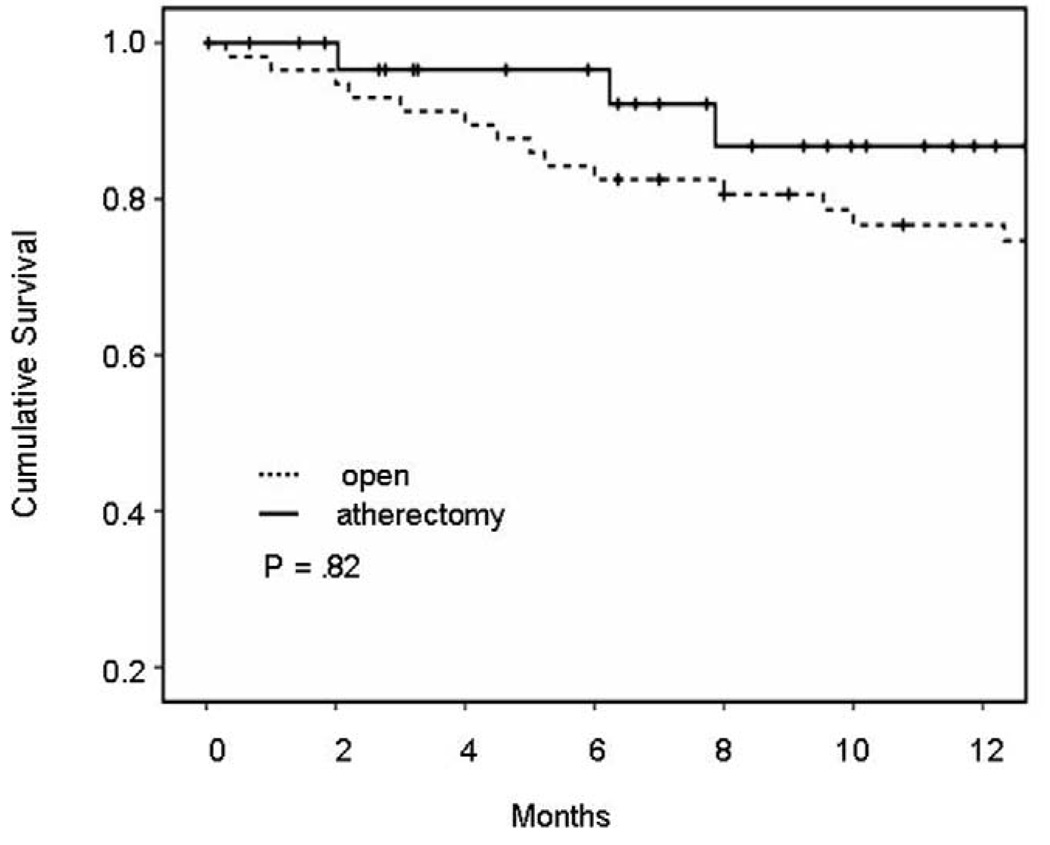
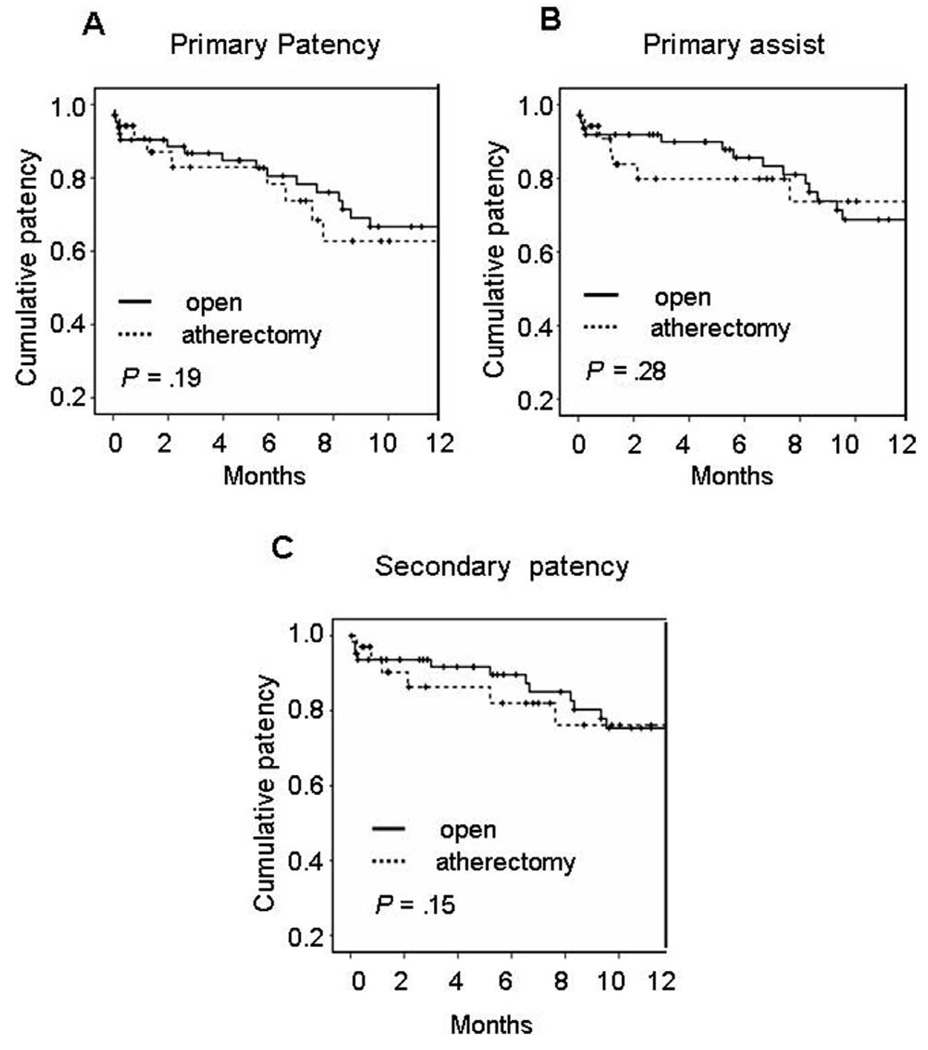
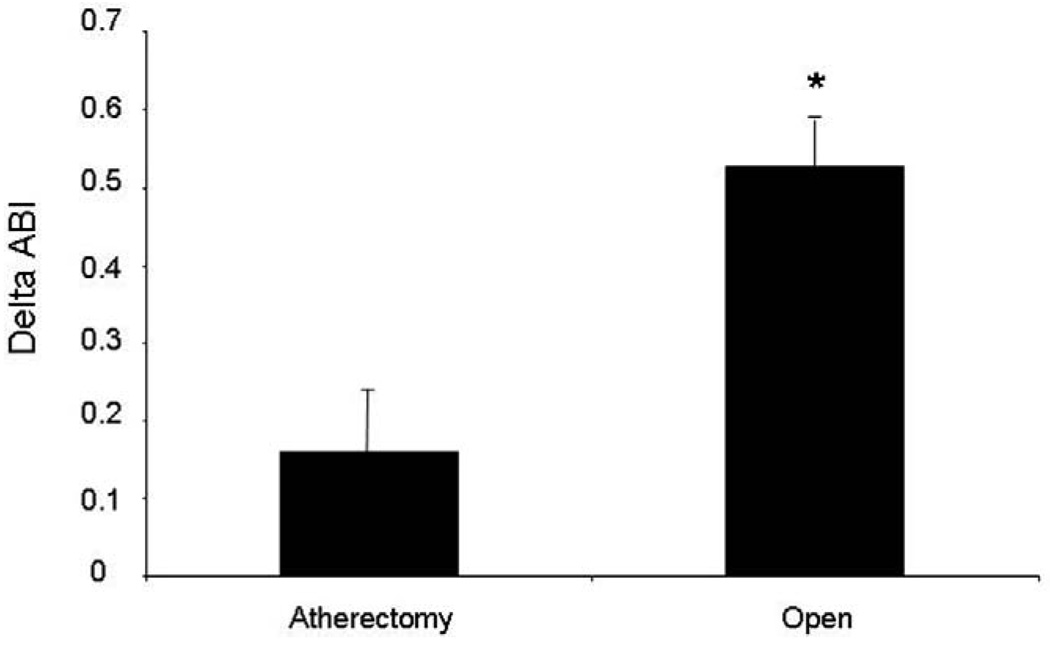
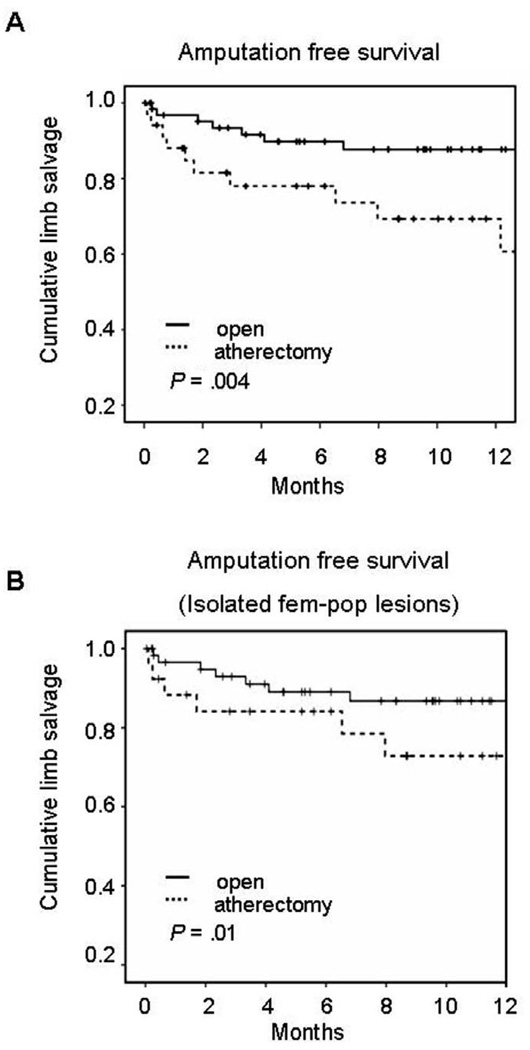
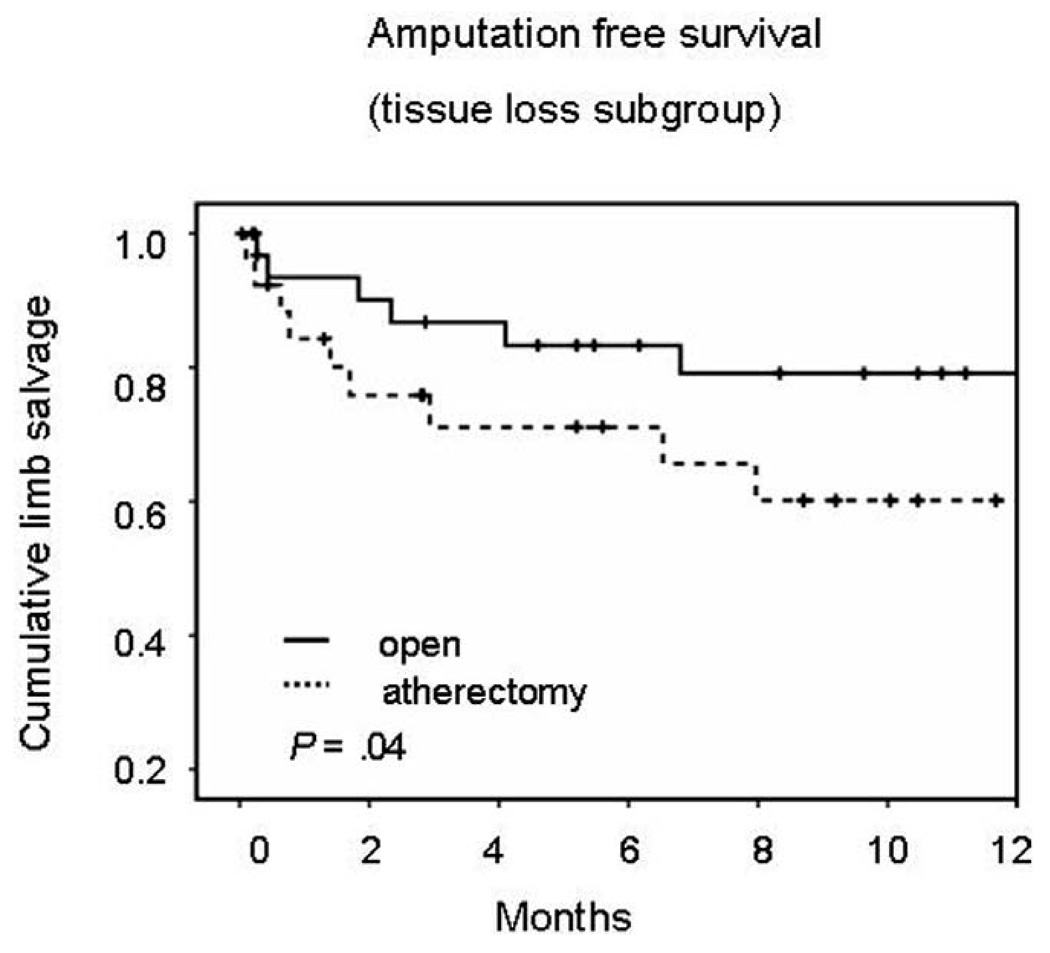
Results: A total of 99 cases involving TASC C (n = 43, 44%) and D (n = 56, 56%) lesions were treated with surgical bypass in 59 patients and atherectomy in 33 patients. Bypass and atherectomy achieved similar 1-year primary patency (64% vs 63%; P = .2). However, the 1-year limb salvage rate was greater in the bypass group (87% vs 69%; P = .004). In the tissue loss subgroup, there was a greater limb salvage rate for bypass patients versus atherectomy (79% vs 60%; P = .04).
Conclusions: Patients with critical limb ischemia may do better with open bypass compared with atherectomy as first-line therapy for limb salvage.
Figures
Similar articles
-
Predictive factors for better bypass patency and limb salvage after prosthetic above-knee bypass reconstruction.J Vasc Surg. 2016 Aug;64(2):380-388.e1. doi: 10.1016/j.jvs.2016.02.059. J Vasc Surg. 2016. PMID: 27763266
-
Reoperative lower extremity revascularization with cadaver vein for limb salvage.Ann Vasc Surg. 2009 Jan-Feb;23(1):24-31. doi: 10.1016/j.avsg.2008.04.011. Epub 2008 Jul 26. Ann Vasc Surg. 2009. PMID: 18657383
-
Atherectomy offers no benefits over balloon angioplasty in tibial interventions for critical limb ischemia.J Vasc Surg. 2013 Oct;58(4):941-8. doi: 10.1016/j.jvs.2013.04.024. Epub 2013 Jun 4. J Vasc Surg. 2013. PMID: 23755978
-
Acute ischemia and bypass occlusion: current options.J Cardiovasc Surg (Torino). 2014 Apr;55(2 Suppl 1):187-94. J Cardiovasc Surg (Torino). 2014. PMID: 24796913 Review.
-
Bypass surgery for lower extremity limb salvage: vein bypass.Methodist Debakey Cardiovasc J. 2012 Oct-Dec;8(4):37-42. doi: 10.14797/mdcj-8-4-37. Methodist Debakey Cardiovasc J. 2012. PMID: 23342187 Free PMC article. Review.
Cited by
-
The role of directional atherectomy in critical-limb ischemia.Ther Adv Cardiovasc Dis. 2021 Jan-Dec;135:17539447211046953. doi: 10.1177/17539447211046953. Ther Adv Cardiovasc Dis. 2021. PMID: 34796770 Free PMC article. Review.
-
Amputation and limb salvage following endovascular and open surgery for the treatment of peripheral artery illnesses: A meta-analysis.Int Wound J. 2023 Nov;20(9):3558-3566. doi: 10.1111/iwj.14229. Epub 2023 Jun 16. Int Wound J. 2023. Retraction in: Int Wound J. 2025 Feb;22(2):e70207. doi: 10.1111/iwj.70207. PMID: 37328950 Free PMC article. Retracted.
References
-
- Norgren L, Hiatt WR, Dormandy JA, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II) J Vasc Surg. 2007;45 suppl S:S5–S67. - PubMed
-
- Norgren L, Hiatt WR, Dormandy JA, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II) Eur J Vasc Endovasc Surg. 2007;33 suppl 1:S1–S75. - PubMed
-
- Norgren L, Hiatt WR, Dormandy JA, et al. Inter-society consensus for the management of peripheral arterial disease. Int Angiol. 2007;26(2):81–157. - PubMed
-
- Albers M, Romiti M, Braganca Pereira CA, Fonseca RL, da Silva Júnior M. A meta-analysis of infrainguinal arterial reconstruction in patients with end-stage renal disease. Eur J Vasc Endovasc Surg. 2001;22(4):294–300. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
