

Right ventricular peak systolic longitudinal strain is a sensitive marker for right ventricular deterioration in adult patients with tetralogy of Fallot
- PMID: 19642012
- PMCID: PMC2729418
- DOI: 10.1007/s10554-009-9477-7
Right ventricular peak systolic longitudinal strain is a sensitive marker for right ventricular deterioration in adult patients with tetralogy of Fallot
Abstract
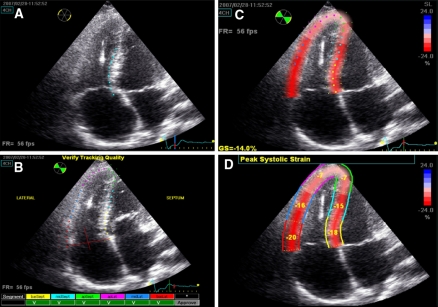
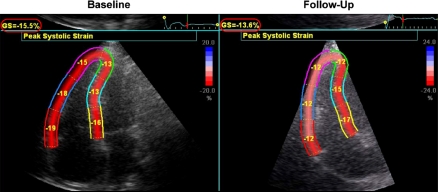
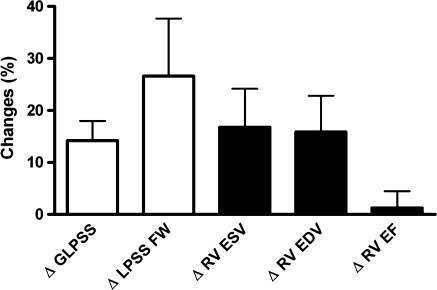
The aim of this study was to evaluate the feasibility of right ventricular (RV) longitudinal peak systolic strain (LPSS) assessment for the follow-up of adult patients with corrected tetralogy of Fallot (TOF). Adult patients (n = 18) with corrected TOF underwent echocardiography and CMR twice with a time interval of 4.2 +/- 1.7 years. RV performance was derived from CMR, and included RV volumes and ejection fraction (EF). LPSS was calculated globally (GLPSS) and in the RV free wall (LPSS FW), with echocardiographic speckle-tracking strain-analysis. Baseline (G)LPSS values were compared between patients and healthy controls; the relation between (G)LPSS and CMR parameters was evaluated and the changes in (G)LPSS and CMR parameters during follow-up were compared. GLPSS and LPSS FW were significantly reduced in patients as compared to controls (-14.9 +/- 0.7% vs. -21.6 +/- 0.9% and -15.5 +/- 0.9% vs. -22.7 +/- 1.5%, P < 0.01). Moderate agreement between LPSS and CMR parameters was observed. RV EF remained unchanged during follow-up, whereas GLPSS and LPSS FW demonstrated a significant reduction. RVEF showed a 1% increase, whereas GLPSS decreased by 14%, and LPSS FW by 27%. RV LPSS is reduced in TOF patients as compared to controls; during follow-up RV EF remained unchanged whereas LPSS decreased suggesting that RV LPSS may be a sensitive marker to detect early deterioration in RV performance.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
