

Focal treatment or observation of prostate cancer: pretreatment accuracy of transrectal ultrasound biopsy and T2-weighted MRI
- PMID: 19643467
- PMCID: PMC3651887
- DOI: 10.1016/j.urology.2009.04.061
Focal treatment or observation of prostate cancer: pretreatment accuracy of transrectal ultrasound biopsy and T2-weighted MRI
Abstract
Objectives: To test the hypothesis that men with prostate cancer (PCA) and preoperative disease features considered favorable for focal treatment would be accurately characterized with transrectal biopsy and prostate magnetic resonance imaging (MRI) by performing a retrospective analysis of a selected cohort of such patients treated with radical prostatectomy (RP).
Methods: A total of 202 patients with PCA who had preoperative MRI and low-risk biopsy criteria (no Gleason grade 4/5, 1 involved core, < 2 mm, PSA density < or = 0.10, clinical stage < or = T2a) were included in the study. Indolent RP pathology was defined as no Gleason 4/5, organ confined, tumor volume < 0.5 mL, and negative surgical margins. MRI ability to locate and determine the tumor extent was assessed.
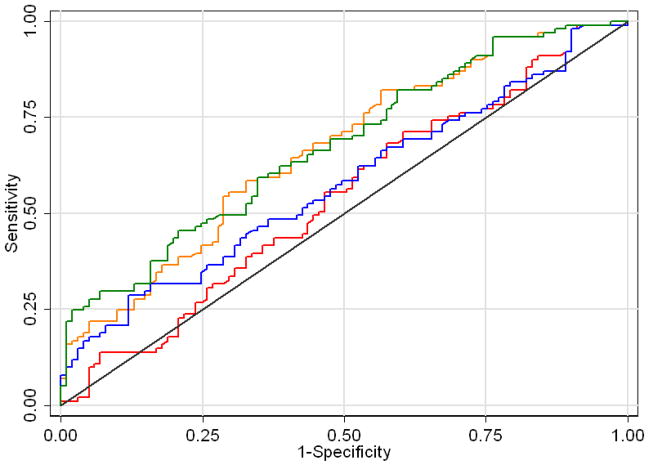
Results: After RP, 101 men (50%) had nonindolent cancer. Multifocal and bilateral tumors were present in 81% and 68% of patients, respectively. MRI indicated extensive disease in 16 (8%). MRI sensitivity to locate PCA ranged from 2% to 20%, and specificity from 91% to 95%. On univariate analysis, MRI evidence of extracapsular extension (P = .027) and extensive disease (P = .001) were associated with nonindolent cancer. On multivariate analysis, only the latter remained as significant predictor (P = .0018).
Conclusions: Transrectal biopsy identified men with indolent tumors favorable for focal treatment in 50% of cases. MRI findings of extracapsular extension and extensive tumor involving more than half of the gland are associated with unfavorable features, and may be useful in excluding patients from focal treatment. According to these data, endorectal MRI is not sufficient to localize small tumors for focal treatment.
2010 Elsevier Inc. All rights reserved.
Figures
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer Statistics, 2008. CA Cancer J Clin. 2008;58:71–96. - PubMed
-
- Carroll PR. Early stage prostate cancer--do we have a problem with over-detection, overtreatment or both? J Urol. 2005;173:1061–1062. - PubMed
-
- Cooperberg MR, Moul JW, Carroll PR. The changing face of prostate cancer. J Clin Oncol. 2005;23:8146–8151. - PubMed
-
- Eggener SE, Scardino PT, Carroll PR, et al. Focal therapy for localized prostate cancer: a critical appraisal of rationale and modalities. J Urol. 2007;178:2260–2267. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
