

Association of blood pressure increases during hemodialysis with 2-year mortality in incident hemodialysis patients: a secondary analysis of the Dialysis Morbidity and Mortality Wave 2 Study
- PMID: 19643520
- PMCID: PMC2767411
- DOI: 10.1053/j.ajkd.2009.05.012
Association of blood pressure increases during hemodialysis with 2-year mortality in incident hemodialysis patients: a secondary analysis of the Dialysis Morbidity and Mortality Wave 2 Study
Abstract
Background: Intradialytic increases in blood pressure (BP) can complicate the management of hypertension in hemodialysis (HD) patients. However, the long-term consequences are uncertain. Thus, we sought to determine whether BP increases during HD were associated with greater 2-year mortality in incident HD patients.
Study design: Secondary analysis of a prospective dialysis cohort.
Setting & participants: Incident HD patients in the Dialysis Morbidity and Mortality Wave 2 Study.
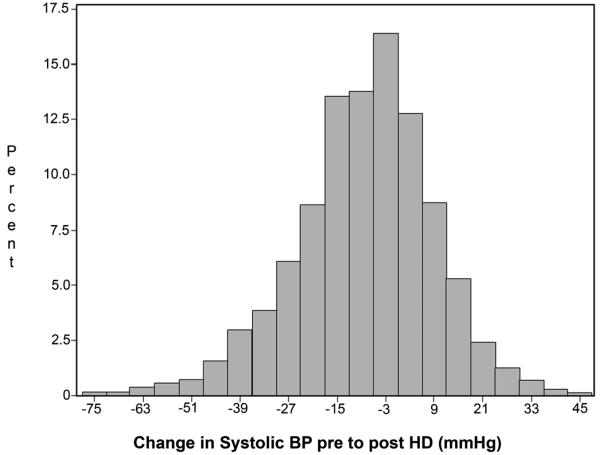
Predictors: Changes in systolic BP (SBP) during HD (ie, postdialysis SBP -- predialysis SBP), averaged from 3 HD sessions before enrollment.
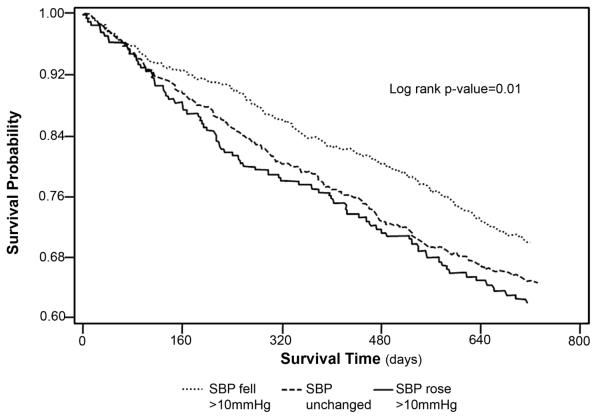
Outcome: Time to 2-year all-cause mortality.
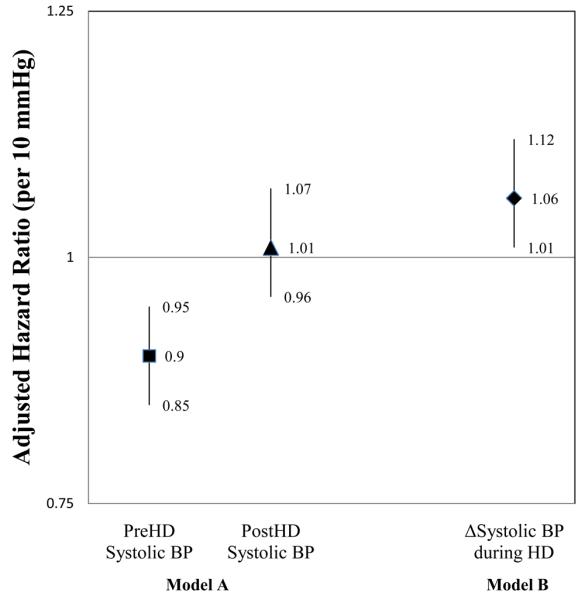
Measurements: Cox regression was used to model hazard ratios for mortality associated with changes in SBP during HD while adjusting for demographics, comorbid conditions, interdialytic weight gain, laboratory variables, and antihypertensive agents.
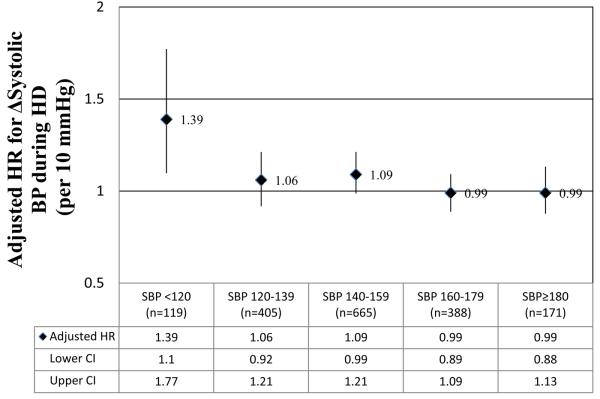
Results: Of 1,748 patients, 12.2% showed greater than 10-mm Hg increases in SBP during HD. In adjusted analyses, every 10-mm Hg increase in SBP during HD was associated independently with a 6% increased hazard of death (hazard ratio, 1.06; 95% confidence interval, 1.01 to 1.11). When also adjusted for diastolic BP and postdialysis SBP, the adjusted hazard of death associated with increasing SBP during HD remained significant (hazard ratio, 1.12; 95% confidence interval, 1.05 to 1.21 per 10-mm Hg increase in SBP during HD). However, in analyses adjusted for predialysis SBP, there was a significant interaction between change in SBP and predialysis SBP. In analyses stratified by predialysis SBP, trends for increased mortality associated with increasing SBP during dialysis were present in patients with predialysis SBP less than 160 mm Hg. However, this relationship was significant only in patients with predialysis SBP less than 120 mm Hg.
Limitations: Secondary analysis with a limited number of baseline BP measurements and limited information about dialysis prescription.
Conclusions: Increasing SBP by more than 10 mm Hg during HD occurs in approximately 10% of incident patients, and although increasing SBP during HD was associated with decreased 2-year survival, these findings were limited to patients with predialysis SBP less than 120 mm Hg.
Figures
Comment in
-
Peridialytic, intradialytic, and interdialytic blood pressure measurement in hemodialysis patients.Am J Kidney Dis. 2009 Nov;54(5):788-91. doi: 10.1053/j.ajkd.2009.07.004. Am J Kidney Dis. 2009. PMID: 19853196 Free PMC article. No abstract available.
References
-
- Shoji T, Tsubakihara Y, Fujii M, Imai E. Hemodialysis-associated hypotension as an independent risk factor for two-year mortality in hemodialysis patients. Kidney Int. 2004;66:1212–1220. - PubMed
-
- Chen J, Gul A, Sarnak MJ. Management of intradialytic hypertension: the ongoing challenge. Semin Dial. 2006;19:141–145. - PubMed
-
- Chou KJ, Lee PT, Chen CL, et al. Physiological changes during hemodialysis in patients with intradialysis hypertension. Kidney Int. 2006;69:1833–1838. - PubMed
-
- Raj DS, Vincent B, Simpson K, et al. Hemodynamic changes during hemodialysis: role of nitric oxide and endothelin. Kidney Int. 2002;61:697–704. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
