

Is all "communicating" hydrocephalus really communicating? Prospective study on the value of 3D-constructive interference in steady state sequence at 3T
- PMID: 19643921
- PMCID: PMC7051287
- DOI: 10.3174/ajnr.A1726
Is all "communicating" hydrocephalus really communicating? Prospective study on the value of 3D-constructive interference in steady state sequence at 3T
Abstract
Background and purpose: 3D-constructive interference in steady state (3D-CISS) sequence has been used to assess the CSF pathways. The aim of this study was to investigate the additive value of 3D-CISS compared with conventional sequences in the diagnosis of obstructive membranes in hydrocephalus.
Materials and methods: A total of 134 patients with hydrocephalus underwent MR imaging examination with a 3T unit consisting of turbo spin-echo, 3D-CISS, and cine phase-contrast (cine PC) sequences. 3D-CISS was used to assess obstructive membranes in CSF pathways compared with other sequences. Cine PC, follow-up imaging, and surgical findings were used to confirm obstructive membranes.
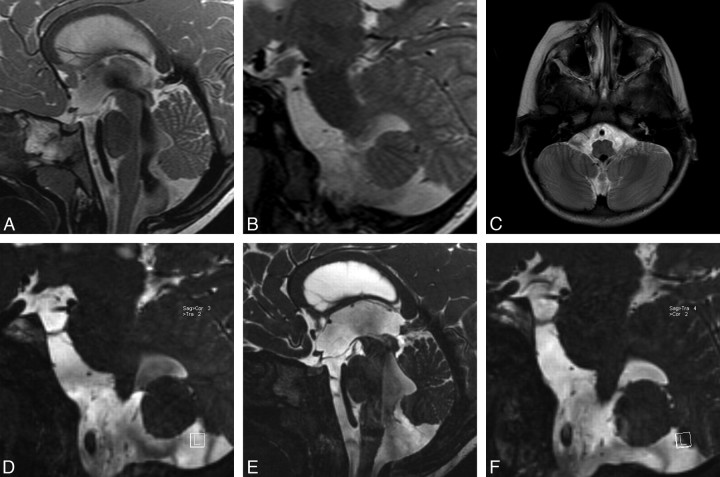
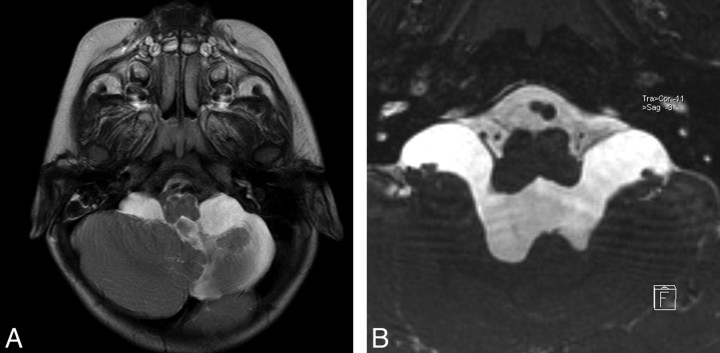
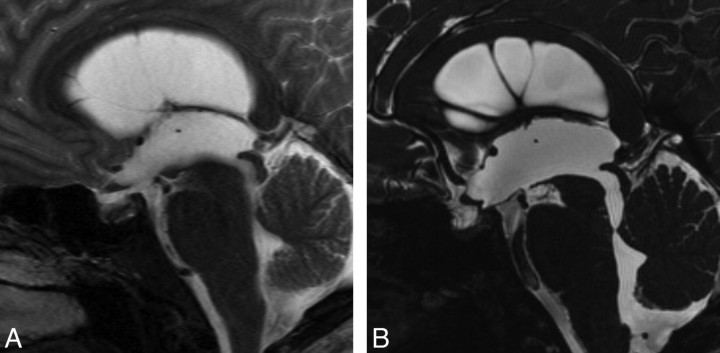
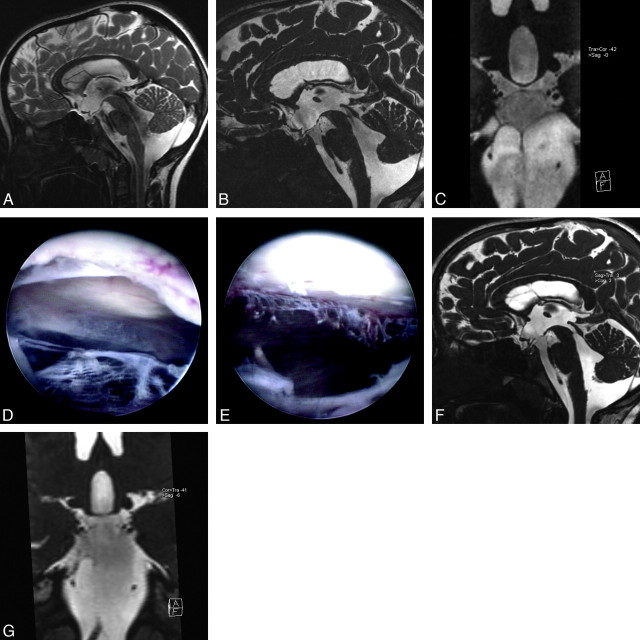
Results: Comparing the number of noncommunicating cases by using the conventional and 3D-CISS images, we found 26 new cases (19.4%) of 134 cases that were previously misdiagnosed as communicating hydrocephalus by conventional images. 3D-CISS sequence identified obstructive membranes invisible in other sequences, which facilitated selection of neuroendoscopy in the treatment of 31 patients (23.1%) in total who would have been otherwise treated with shunt insertion. These patients included 26 newly diagnosed noncommunicating cases after demonstration of intraventricular and/or fourth ventricular outlet membranes and 5 cases of communicating hydrocephalus with obstructing cisternal membranes. There were obstructions of the foramina of Luschka in 22 of 26 newly found noncommunicating cases.
Conclusions: Conventional sequences are insensitive to obstructive membranes in CSF pathways, especially in the fourth ventricular exit foramina and the basal cisterns. 3D-CISS sequence, revealing these obstructive membranes, can alter patient treatment and prognosis.
Figures
Similar articles
-
Three-dimensional constructive interference in steady-state magnetic resonance imaging in obstructive hydrocephalus: relevance for endoscopic third ventriculostomy and clinical results.J Neurosurg. 2008 Nov;109(5):931-8. doi: 10.3171/JNS/2008/109/11/0931. J Neurosurg. 2008. PMID: 18976087
-
Phase-contrast MRI and 3D-CISS versus contrast-enhanced MR cisternography for the detection of spontaneous third ventriculostomy.J Neuroradiol. 2011 May;38(2):98-104. doi: 10.1016/j.neurad.2010.03.006. Epub 2010 Jun 7. J Neuroradiol. 2011. PMID: 20627312
-
Three-Dimensional Constructive Interference in Steady State Sequences and Phase-Contrast Magnetic Resonance Imaging of Arrested Hydrocephalus.World Neurosurg. 2017 Feb;98:296-302. doi: 10.1016/j.wneu.2016.10.140. Epub 2016 Nov 5. World Neurosurg. 2017. PMID: 27826087
-
Noncommunicating Hydrocephalus.Semin Ultrasound CT MR. 2016 Apr;37(2):109-19. doi: 10.1053/j.sult.2015.12.004. Epub 2015 Dec 17. Semin Ultrasound CT MR. 2016. PMID: 27063661 Review.
-
Magnetic resonance imaging of noncommunicating hydrocephalus.World Neurosurg. 2013 Feb;79(2 Suppl):S21.e9-12. doi: 10.1016/j.wneu.2012.02.009. Epub 2012 Feb 10. World Neurosurg. 2013. PMID: 22381823 Review.
Cited by
-
The presence of a foramen of Luschka in the American alligator (Alligator mississippiensis) and the continuity of the intraventricular and subdural spaces.J Anat. 2024 Mar;244(3):391-401. doi: 10.1111/joa.13972. Epub 2023 Nov 15. J Anat. 2024. PMID: 37965891 Free PMC article.
-
Blake's pouch cyst.Surg Neurol Int. 2014 Jul 24;5:112. doi: 10.4103/2152-7806.137533. eCollection 2014. Surg Neurol Int. 2014. PMID: 25101207 Free PMC article. Review.
-
Hydrocephalus in patients with neurofibromatosis type 1: MR imaging findings and the outcome of endoscopic third ventriculostomy.AJNR Am J Neuroradiol. 2011 Apr;32(4):643-6. doi: 10.3174/ajnr.A2357. Epub 2011 Feb 17. AJNR Am J Neuroradiol. 2011. PMID: 21330395 Free PMC article.
-
Hydrocephalus, a rare manifestation of sarcoidosis.Clin Pract. 2011 Sep 30;1(3):e66. doi: 10.4081/cp.2011.e66. eCollection 2011 Jul 1. Clin Pract. 2011. PMID: 24765327 Free PMC article.
-
Diagnostic performance of heavily T2-weighted techniques in obstructive hydrocephalus: comparison study of two different 3D heavily T2-weighted and conventional T2-weighted sequences.Jpn J Radiol. 2015 Feb;33(2):94-101. doi: 10.1007/s11604-014-0385-y. Epub 2015 Jan 7. Jpn J Radiol. 2015. PMID: 25559932
References
-
- Fushimi Y, Miki Y, Ueba T, et al. Liliequist membrane: three-dimensional constructive interference in steady state MR imaging. Radiology 2003;229:360–65 - PubMed
-
- Kakizawa Y, Hongo K, Takasawa H, et al. “Real” three-dimensional constructive interference in steady-state imaging to discern microneurosurgical anatomy. Technical note. J Neurosurg 2003;98:625–30 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical