

Primary extracranial meningiomas: an analysis of 146 cases
- PMID: 19644540
- PMCID: PMC2715454
- DOI: 10.1007/s12105-009-0118-1
Primary extracranial meningiomas: an analysis of 146 cases
Abstract
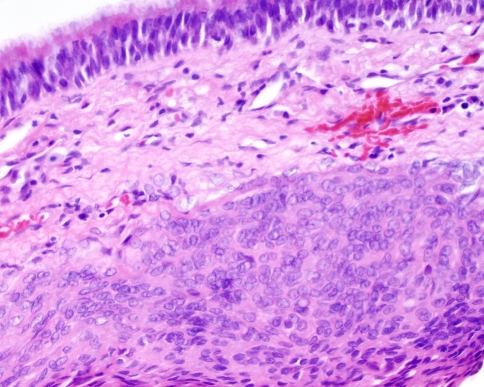
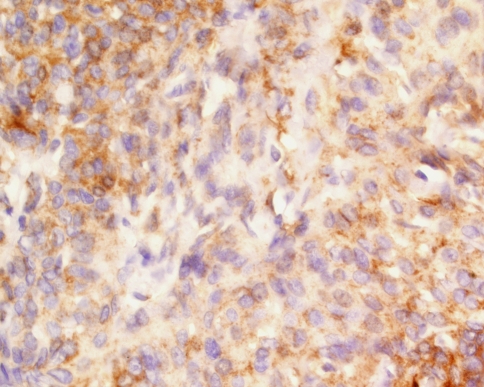
Primary extracranial meningiomas are rare neoplasms, frequently misdiagnosed, resulting in inappropriate clinical management. To date, a large clinicopathologic study has not been reported. One hundred and forty-six cases diagnosed between 1970 and 1999 were retrieved from the files of the Armed Forces Institute of Pathology. Histologic features were reviewed, immunohistochemistry analysis was performed (n = 85), and patient follow-up was obtained (n = 110). The patients included 74 (50.7%) females and 72 (49.3%) males. Tumors of the skin were much more common in males than females (1.7:1). There was an overall mean age at presentation of 42.4 years, with a range of 0.3-88 years. The overall mean age at presentation was significantly younger for skin primaries (36.2 years) than for ear (50.1 years) and nasal cavity (47.1 years) primaries. Symptoms were in general non-specific and reflected the anatomic site of involvement, affecting the following areas in order of frequency: scalp skin (40.4%), ear and temporal bone (26%), and sinonasal tract (24%). The tumors ranged in size from 0.5 up to 8 cm, with a mean size of 2.3 cm. Histologically, the majority of tumors were meningothelial (77.4%), followed by atypical (7.5%), psammomatous (4.1%) and anaplastic (2.7%). Psammoma bodies were present in 45 tumors (30.8%), and bone invasion in 31 (21.2%) of tumors. The vast majority were WHO Grade I tumors (87.7%), followed by Grade II (9.6%) and Grade III (2.7%) tumors. Immunohistochemically, the tumor cells labeled for EMA (76%; 61/80), S-100 protein (19%; 15/78), CK 7 (22%; 12/55), and while there was ki-67 labeling in 27% (21/78), <3% of cells were positive. The differential diagnosis included a number of mesenchymal and epithelial tumors (paraganglioma, schwannoma, carcinoma, melanoma, neuroendocrine adenoma of the middle ear), depending on the anatomic site of involvement. Treatment and follow-up was available in 110 patients: Biopsy, local excision, or wide excision was employed. Follow-up time ranged from 1 month to 32 years, with an average of 14.5 years. Recurrences were noted in 26 (23.6%) patients, who were further managed by additional surgery. At last follow-up, recurrent disease was persistent in 15 patients (mean, 7.7 years): 13 patients were dead (died with disease) and two were alive; the remaining patients were disease free (alive 60, mean 19.0 years, dead 35, mean 9.6 years). There is no statistically significant difference in 5-year survival rates by site: ear and temporal bone: 83.3%; nasal cavity: 81.8%; scalp skin: 78.5%; other sites: 65.5% (P = 0.155). Meningiomas can present in a wide variety of sites, especially within the head and neck region. They behave as slow-growing neoplasms with a good prognosis, with longest survival associated with younger age, and complete resection. Awareness of this diagnosis in an unexpected location will help to avoid potential difficulties associated with the diagnosis and management of these tumors.
Keywords: Extracranial; Immunohistochemistry; Meningioma; Prognosis; Radiation; WHO classification.
Figures
References
-
- Louis DN, Ohgaki H, Wiestler OD, Cavenee WK. World Health Organization classification of tumours of the central nervous system. 4. Lyon: IARC Press; 2007.
-
- Galm T, MacGregor F, Sinclair AM, Hunter J, McPhaden A. Extracranial meningioma presenting as a neck mass in a patient with underlying ankylosing spondylitis. J Rheumatol. 2006;33:1883–1885. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
