

13-cis-retinoic acid re-differentiation therapy and recombinant human thyrotropin-aided radioiodine treatment of non-Functional metastatic thyroid cancer: a single-center, 53-patient phase 2 study
- PMID: 19646277
- PMCID: PMC2739165
- DOI: 10.1186/1756-6614-2-8
13-cis-retinoic acid re-differentiation therapy and recombinant human thyrotropin-aided radioiodine treatment of non-Functional metastatic thyroid cancer: a single-center, 53-patient phase 2 study
Abstract
In 30-50% of patients with metastatic non-medullary thyroid cancer the metastases are not radioiodine-avid and so there is no effective treatment. Retinoids have demonstrated inhibition of thyroid tumor growth and induction of radioiodine uptake. The aim of our study was to assess benefits of the retinoic acid (RA) treatment to re-differentiate non-functional NMTC metastases.
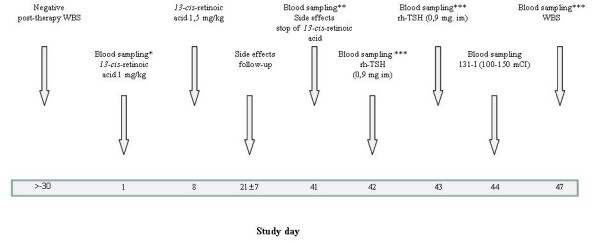
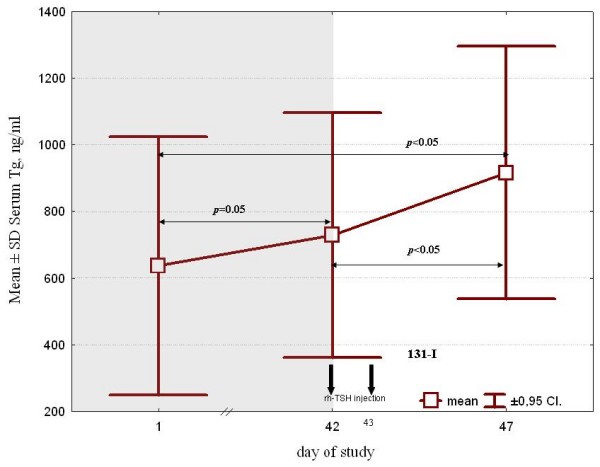
Patients and methods: In this prospective study, 53 patients with radioiodine non avid metastatic disease (45) or hyperthyroglobulinemia (8) were treated with 13-cis-retinoic acid (13-CRA) [1.0 mg/kg/day over 1st week and then 1.5 mg/kg] for six weeks prior to I-131 treatment performed under rhTSH stimulation. The re-differentiating effect of RA was evaluated by serum thyroglobulin (Tg) monitoring before and after cessation of RA treatment and by qualitative analysis of iodine uptake on the post-therapeutic whole body scan (rxWBS).
Results: 13-CRA induced radioiodine uptake in 9 (17%) of patients. In the univariate analysis neither the patient's gender, age, tumor histopathology, uptake in thyroid bed nor time since thyroid cancer diagnosis was associated with results of rxWBS.41 (77%) patients were evaluable for Tg response before and after to 13-CRA treatment. There was a statistically significant increase in median Tg level (60 v. 90 ng/ml, p < 0.05). There was no difference in Tg increase between scintigraphic responders and non-responders.13-CRA and RIT was repeated at least once in 8 of 9 scintigraphic responders. None of them showed tumor regression by radiological imaging within 12 months after the first treatment, 4/9 (44%) of them had disease progression.13-CRA treatment was well-tolerated. All but one patient complained of at least one side effect the most prevalent being lip dryness (98%). All side effects were transient and resolved within 2 weeks after 13-CRA cessation.
Conclusion: Our results show that in patients with non-functional metastases from NMTC, 13-CRA is able to exert some re-differentiation effect by induction of radioiodine uptake in <20% of patients and increase of Tg serum level in about 30% of them. Nevertheless, this does not transfer into clinical benefit as it neither induces measurable tumor response nor prevents disease progression.
Figures
References
-
- Seidlin SM, Marinelli L, Oshry E. Radioactive iodine therapy effect on functioning metastases of adenocarcinoma of thy thyroid gland. JAMA. 1946;132:838–847. - PubMed
-
- Durante C, Haddy N, Baudin E, Leboulleux S, Hartl D, Travagli JP, Caillou B, Ricard M, Lumbroso JD, De Vathaire F, Schlumberger M. Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: benefits and limits of radioiodine therapy. J Clin Endocrinol Metab. 2006;91:2892–2899. doi: 10.1210/jc.2005-2838. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
