

Persistence of HIV-1 receptor-positive cells after HSV-2 reactivation is a potential mechanism for increased HIV-1 acquisition
- PMID: 19648930
- PMCID: PMC2723183
- DOI: 10.1038/nm.2006
Persistence of HIV-1 receptor-positive cells after HSV-2 reactivation is a potential mechanism for increased HIV-1 acquisition
Abstract
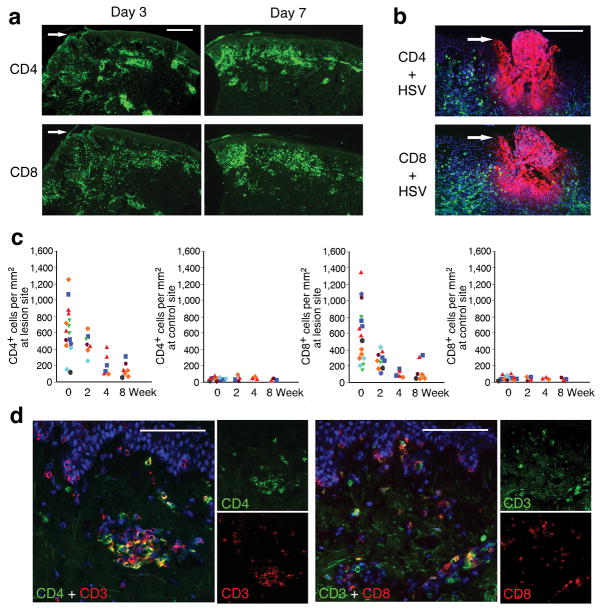
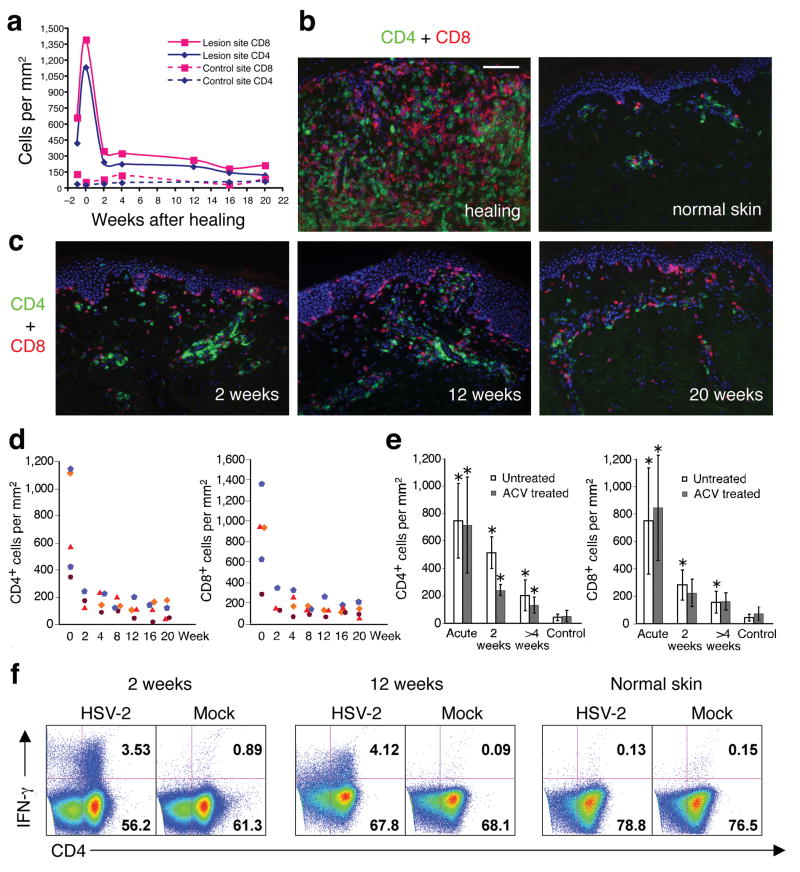
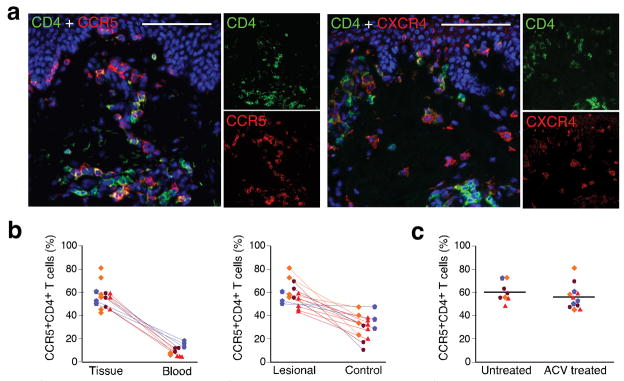
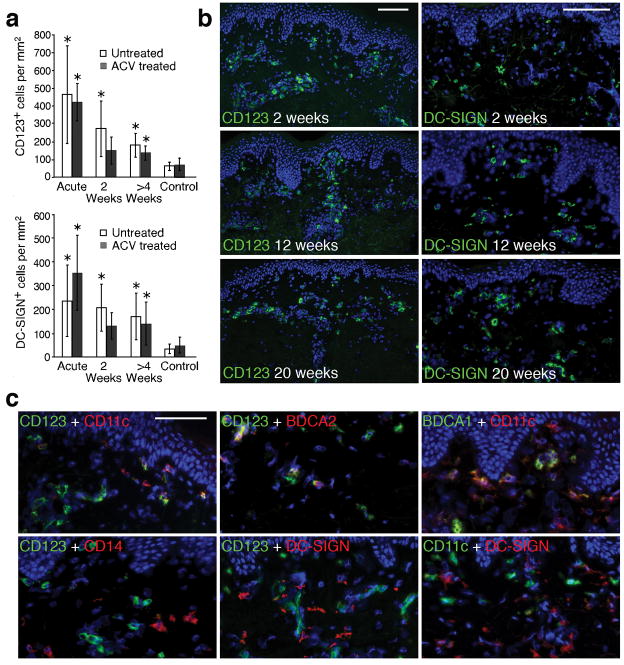
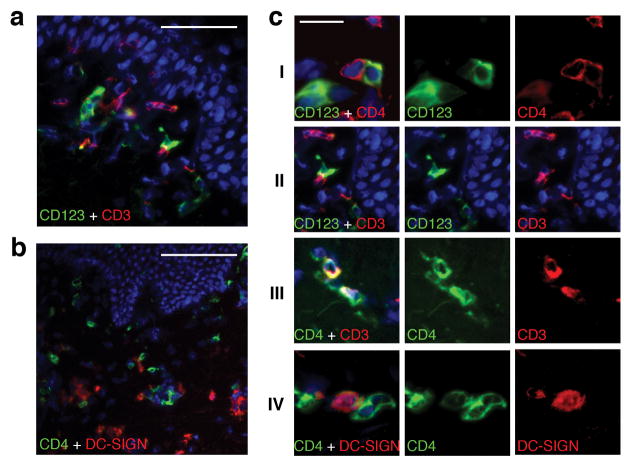
To explore the mechanism by which herpes simplex virus (HSV)-2 infection is related to HIV-1 acquisition, we conducted in situ analysis of the cellular infiltrate from sequential biopsies of HSV-2 lesions from patients on and off antiviral therapy. CD4(+) and CD8(+) T cells and a mixed population of plasmacytoid and myeloid dendritic cells (DCs), including cells expressing the C-type lectin receptor DC-SIGN, persisted at sites of HSV-2 reactivation for months after healing, even with daily antiviral therapy. The CD4(+) T cells that persisted reacted to HSV-2 antigen, were enriched for expression of the chemokine receptor CCR5, and were contiguous to DCs expressing the interleukin-3 receptor CD123 or DC-SIGN. Ex vivo infection with a CCR5-tropic strain of HIV-1 revealed greater concentrations of integrated HIV-1 DNA in cells derived from healed genital lesion biopsies than in cells from control skin biopsies. The persistence and enrichment of HIV receptor-positive inflammatory cells in the genitalia help explain the inability of anti-HSV-2 therapy to reduce HIV acquisition.
Figures
References
-
- Freeman EE, et al. Herpes simplex virus 2 infection increases HIV acquisition in men and women: systematic review and meta-analysis of longitudinal studies. Aids. 2006;20:73–83. - PubMed
-
- Wald A, Link K. Risk of Human Immunodeficiency Virus (HIV) Infection in Herpes Simplex Virus Type-2 (HSV-2) Seropositive Persons: a Meta-Analysis. J Infect Dis. 2002;185:45–52. - PubMed
-
- Gupta R, et al. Valacyclovir and acyclovir for suppression of shedding of herpes simplex virus in the genital tract. J Infect Dis. 2004;190:1374–1381. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
